Fig. 12.1
Hip hinge distraction external fixator (Smith and Nephew Modular Rail System) supine (a) and sitting (b)
The patient is positioned supine with no bump under the hip. The pelvis should remain level and not tilted toward one side or another. The entire forequarter of the limb, from midline anterior to midline posterior and from ribs to toes, was prepped and draped free.
Step 1: Arthrogram of hip joint.
Anteroposterior and frog leg views are obtained with arthrographic dye in place.
Step 2: Percutaneous adductor tenotomy of adductor longus and gracilis tendons.
Step 3: Psoas tenotomy
Make a 3–4 cm anterior groin line incision. Feel the femoral artery pulse and stay lateral to it. Identify the medial border of the sartorius muscle and dissect deep and medial to it. The femoral nerve is identified and retracted medially. The nerve lies on the medial anterior aspect of the iliopsoas muscle. Dissect down the medial side of this muscle, and on the undersurface of its medial side can be found the psoas tendon. Cut the tendon while leaving a continuous muscle bridge.
Step 4: Insert a flexion-extension axis pin into the femoral head.
A horizontal line of the pelvis is marked on the drapes, guided by the image intensifier (line across the top of both iliac crests or bottom of both ischial tuberosities). The affected lower limb is held with the patella forward, knee in extension, and hip in 15° of abduction relative to the horizontal line of the pelvis. With the image intensifier and a wire, mark a line over the shaft of the femur and a point over the center of the acetabulum. Draw a line from the center of the acetabulum point, perpendicular to the shaft of the femoral line. Place the image intensifier into the lateral view. The dye in the hip joint helps identify the circumference of the femoral head. Draw a line representing the equator of the femoral head in the sagittal plane. Insert a 2.5 mm Steinmann pin into the center of the femoral head from the intersection point of the AP line with the lateral line. These pins should be perpendicular to the shaft of the femur, end in the center of the acetabulum, and be in the midsagittal plane of the femoral head. Because the hip is usually proximally migrated, the center of rotation of the femoral head will be proximal to the center of the acetabulum. The axis pins should be centered on the acetabulum and is therefore more distal to the center of the femoral head.
Step 5: Preconstruct a hinged monolateral external fixator (e.g., Orthofix, EBI, or the SN modular rail system (MRS)) and apply the cannulated hinge over the axis pin.
Step 6: Insert the femoral frontal plane pins.
Adjust the distal clamp to the level desired on the femur. Insert two frontal plane pins with the femur kept in the patella forward position. Leave room for lengthening on the distal fixator.
Step 7: Insert two pins into the anterolateral pelvis.
Roll the operating room table to the opposite side and place the image intensifier over the affect supra-acetabular region. When a triangle is visualized over the acetabulum, the correct plane for the pin is seen. Drill a 1.8 mm wire into this triangle and then tap it in until a hollow sound from hitting a cortex is heard. If the wire is in the correct plane, then level the table and overdrill the wire with a 4.8 mm cannulated drill bit or in smaller children a 3.2 mm cannulated drill bit. Insert a hydroxyapatite-coated half-pin. Repeat the same for a pin either more proximal or more distal to the first.
Step 8: Attach an arch to these first two pins so that the arch is in line with the rest of the fixator based on the constraints of the fixator.
This arch will usually not be perpendicular to the pelvis due to the 15° abduction of the hip joint.
Step 9: Add one transverse and one oblique pin to the pelvic arch for a total of 4 pins in the pelvis. The transverse pin should be in the supra-acetabular region. The oblique pin should be between the transverse and the two anterior pins.
Step 10: Test the hip motion. The hip should move easily in flexion-extension.
Step 11: Perform an acute distraction of the hip joint so that Shenton line is over reduced.
Step 12: Reduce any lateral subluxation of the hip. This is achieved by loosening the fixation of the distal frontal plane pins and pushing the femur medially to reduce the femoral head deeper into the acetabulum.
Step 13: Insert one or two more distal femoral pins in a delta configuration to the frontal plane pins.
Step 14: Add an arch to the distal femur clamp.
Step 15: Add a removable distraction rod anteriorly between the pelvic arch and the distal femoral arch to prevent flexion contracture by keeping the hip extended especially at night.
12.1.3 Postoperative Management of Distraction Treatment for Perthes Disease
Physiotherapy is initiated immediately to work on hip flexion-extension, with emphasis on maintaining hip extension with prone exercises. The therapist must clearly understand that they are not to work on hip abduction, adduction, external rotation, or internal rotation because this would stress the external fixation pin-bone interface. The patient and therapist are taught to measure the true hip motion at the hip hinge rather than doing so clinically (i.e., between the thigh and the spine). The patient is taught how to perform flexion-extension exercises at home, supplementing the hour of daily physical therapy. Patients are allowed 50 % weight bearing while the external fixator is in place.
Flexion contracture of the hip commonly develops. Physiotherapy is important for prevention and treatment of contractures. If a severe degree of flexion contracture occurs, distraction of the hip joint is compromised. Using the removable hip extension bar prevents this complication. The apparatus is left in place for 4 months in patients younger than 12 years and for 5 months in patients 12 years and older. This usually correlates with radiograph re-ossification of the lateral pillar.
Apparatus removal is performed under general anesthesia as an outpatient procedure. Because of the osteoporosis of the femoral head and neck, manipulation of the hip with the patient under anesthesia should not be performed after the removal to avoid fracture of the hip or femur. A bilateral abduction brace (pelvic band with bilateral thigh cuffs and hip hinges) set at 30° of abduction per leg is applied after the removal and was used both day and night for 6 weeks. Resumption of full weight bearing begins on a gradual basis immediately after fixator removal, and full weight bearing is achieved in approximately 4 weeks. After 6 weeks of full-time use, the abduction splint is used only at night for 6 months. Running, jumping, and participation in sports are not allowed for 1 year after treatment. Swimming, cycling, and walking are encouraged. The patient is taught a series of five stretches I call the Perthes exercises. These should be performed twice daily until skeletal maturity.
Perthes Exercises
1.
Wide abduction standing
2.
Supine hip flexion
3.
Prone internal rotation stretches
4.
Prone external rotation stretches
5.
Prone hyperextension of the hip
12.1.4 Results
Paley and Segev conducted a retrospective study of the first 16 consecutive patients (18 hips) treated by hip joint distraction between July 1989 and July 1999. Fourteen patients had Perthes disease, and two had avascular necrosis of the hip after slipped capital femoral epiphysis. The patient group was comprised of four girls and 12 boys. Two patients had bilateral hip involvement and received the same treatment for both hips. One patient received repeat distraction treatment of the same hip. The mean patient age at the time of disease onset was 9.1 years (range, 6–14 years). The mean patient age at the time of surgery was 10.2 years (range, 6.5–15.6 years). All patients with Perthes disease had whole-head involvement, and the cases were classified as Catterall IV (Catterall 1971; Lloyd-Roberts et al. 1976; Herring et al. 1992; Salter and Thompson 1984) or depending on the date of initial presentation to the senior author. The two patients with slipped capital epiphysis experienced collapse of the femoral head resulting from avascular necrosis.
The treatment protocol used in all these cases was based on previous experience with hip distraction for chondrolysis and hip dislocation and the successful treatment of the first patient in this series in 1989 (Fig. 12.2 ). Containment surgery by osteotomy was contraindicated for this 11-year-old patient who presented with a very stiff, subluxed, and deformed hip that had previously been treated by bracing for 1 year. Distraction was proposed to reduce the hip, which had marked proximal migration and subluxation. This patient was considered to have a very poor prognosis before treatment. The striking success of the distraction treatment in this difficult case encouraged us to offer distraction treatment as an alternative therapy for patients who subsequently presented with Perthes disease. Conventional treatment options, such as pelvic and femoral osteotomy and shelf procedures, were discussed with all patients and were offered as surgical management options when patients met the criteria for these procedures. The surgical approach and treatment protocol for all patients treated by distraction was identical to those used for the index patient, and all documentation was conducted in the same way at the same time intervals. Although this study is retrospective in that no formal study was organized or planned in advance, all the data were collected for clinical documentation in a prospective fashion by the treating author. These data were later reviewed for this retrospective study.
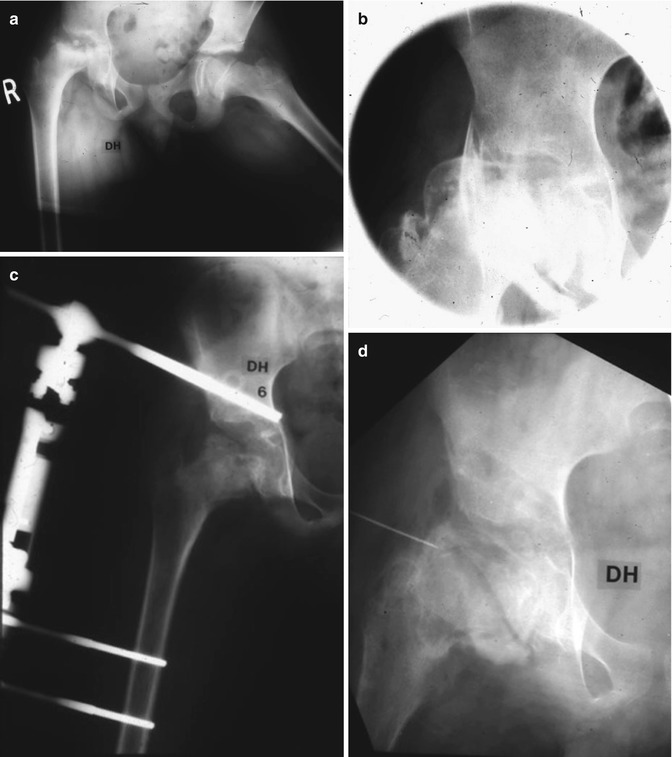
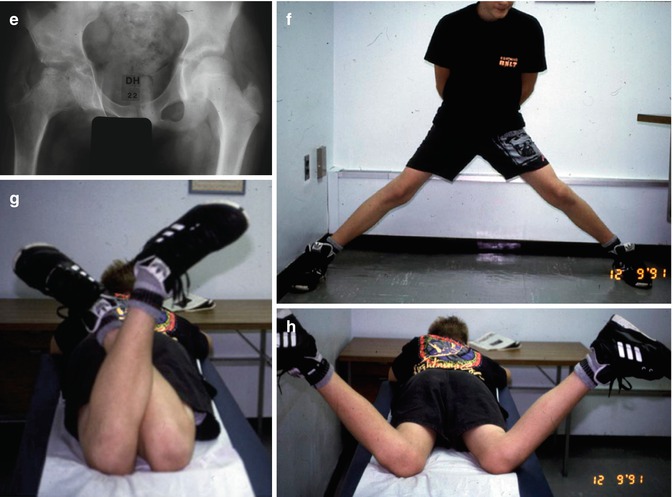

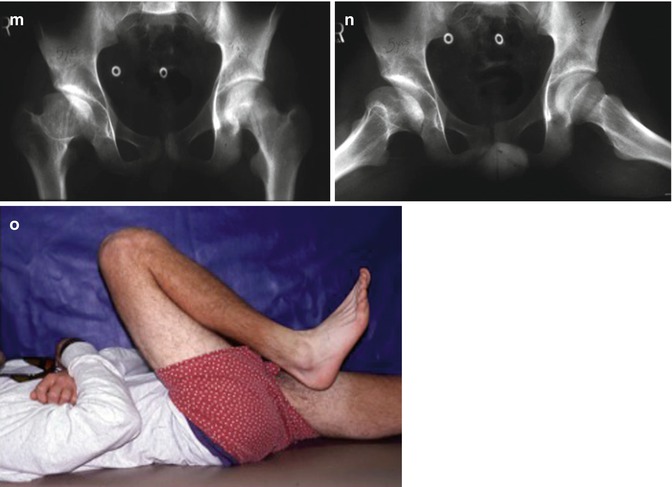
Fig. 12.2
(a) An 11-year-old boy with Perthes with fixed flexion-adduction contracture. There is a break in Shenton line with proximal and lateral migration of the femoral head; (b) intraoperative arthrogram showing femoral head flattening; (c) reduction of the femoral head by application of hinge distraction external fixator with hip in 15° of abduction; (d) arthrogram at time of removal of apparatus. The femoral head is rounder; (e) follow-up radiograph 22 months after surgery; (f) hip abduction 22 months after distraction; hip external (g) and internal (h) rotation 22 months after distraction; hip abduction 10 years after distraction (i, j); hip external (k) and internal (l) rotation 22 months after distraction; AP (m) and frog lateral (n) pelvis x-rays 10 years after distraction; flexion 10 years after distraction (o)
The families of all patients who were offered the distraction treatment were first given the phone numbers of one or two previously treated patients so that they could contact them. Families made their decision to proceed with distraction or containment surgical treatment based on their conversations with previous patients and based on information provided by the surgeon regarding conventional treatment. Because of our success in the treatment of Perthes disease, the distraction regimen was additionally applied to all cases of avascular necrosis resulting from slipped capital femoral epiphysis treated during the same time period. To date, all these patients have chosen distraction treatment.
External fixation was in use at our institution for hip joint distraction and distraction of other joints for various indications; the use of the technique to treat Perthes disease was therefore not considered experimental. During the study period, internal review board approval was not required by our institution for the application of hip distraction to cases of Perthes disease or avascular necrosis of the hip. Furthermore, because no formal prospective study was being conducted, this study is considered retrospective. Internal review board approval was obtained to conduct this retrospective study.
All patients, while under general anesthesia, underwent intraoperative arthrography of the hip at the time of external fixator application and post-distraction arthrography of the hip at the time of fixator removal. Patients were examined every 6 months for the first 2 years and then annually for the remainder of the study period. Clinical observations were evaluated and recorded by the senior author at each follow-up visit and included subjective pain and activity levels, bilateral hip range of motion (flexion, fixed flexion deformity, abduction, adduction, prone internal, and external rotation), knee range of motion, Trendelenburg test, clinical gait assessment, and anteroposterior plus frog leg view pelvic radiographs. The average time from surgery to most recent follow-up visit was 6.7 years (range, 3.5–13.4 years). The clinical evaluations and final follow-up radiographs were tabulated and analyzed.
Based on the total arc of hip range of motion, a clinical sphericity index was calculated to describe how close the hip motion was to being spherical. This index was calculated by dividing the total arc of motion in all three planes of motion (flexion-extension, abduction-adduction, and internal-external rotation) of the diseased hip by 270°, which is the average normal total hip range of motion. The clinical sphericity index is expressed as a percentage of normal total range of motion. The hip was considered to move spherically if the index was greater than two-thirds (67 %) of the normal range.
We also calculated the sphericity of the femoral head using measurements derived from pre- and post-distraction arthrograms. The ratios between the largest diameter of the femoral head divided by the lesser diameter (two times the lesser radius, perpendicular to the largest diameter, and bisecting it in its middle), on the anteroposterior and lateral view arthrograms, were added together and divided by 2 to calculate an index. A normal index for a spherical femoral head is 1.1 (Bennett et al. 2002). The closer the index is to 1.1, the more spherical is the head. The initial and final arthrogram ratios were compared.
The final follow-up radiographs, including those of patients who were not skeletally mature, were graded using the Stulberg et al. (1981) classification system. The following radiographic parameters were measured on the preoperative and final radiographs for the operated and normal hips: sharp acetabular angle, central edge angle, proximal migration of Shenton line, and distance of the medial border of the femoral head from the tear drop. Closure of the proximal femoral physis on the normal side was noted and considered to be evidence of hip skeletal maturity. A premature closure of the diseased hip physis relative to the normal hip also was noted.
Fifteen patients had complained of varying degrees of pain before surgery. At final follow-up, only one patient complained of mild pain that did not require analgesics and did not interfere with daily activities. All patients returned to full school and/or work activities, including sports without limitation. All patients expressed satisfaction with the results and indicated vast improvement in their function compared with their pretreatment abilities. Fifteen patients walked with a limp before the operation, compared with only one patient who walked with mild lurch gait at final follow-up. Fifteen patients had positive Trendelenburg sign before the operation, compared with only one with positive Trendelenburg sign at final follow-up. All patients had full ipsilateral knee range of motion before surgery and at final follow-up.
All our patients experienced marked limitation of motion on the affected side at presentation. At final follow-up, the mean flexion-extension arc of motion was 100° (range, 90–130°). The mean abduction-adduction arc of motion was 54° (range, 25–75°). The mean internal-external rotation arc of motion was 58° (range, 0–90°). The mean total hip arc of motion was 214° (range, 115–285°). The mean arc of motion for the treated hip was 79 % of normal (range, 43–100 %). At final follow-up, 16 of 18 hips that underwent hip joint distraction had their range of motion restored to at least two-thirds normal; two hips had a range of motion below functional range.
During distraction, early, rapid osteoporosis of the femoral head was consistently observed, revealing sclerotic dead bone. This was followed by gradual ossification of the lateral pillar, which usually was completed by 4 months. All patients except two underwent external fixator application after femoral head collapse and during the resorption phase. Two patients underwent application of the external fixator just after the initial subchondral fracture. In both of these cases, the femoral head re-collapsed after fixator removal and subsequently went through a resorption phase. One of these patients underwent a second distraction treatment, and complete success was achieved the second time.
At the most recent follow-up visit, nine patients had reached skeletal maturity as judged by closure of the femoral capital epiphysis in the normal hip. Three hips showed signs of premature physeal closure on the operated side. The mean preoperative Sharp acetabular angle was 45° (range, 40–50°) and at final follow-up was 44° (range, 35–50°). The mean preoperative center-edge angle was 19° (range, 0–30°) and increased to 24° (range, 15–35°) postoperatively. The difference between pre- and postoperative Sharp acetabular angles was not significant (P = 0.094); the increase in the center-edge angle after treatment was marginally significant (P = 0.051).
The mean proximal migration measured as a break in Shenton line was 7 mm (range, 0–14 mm) preoperatively and improved to 2 mm (range, 0–12 mm) at the most recent follow-up visit. This difference was statistically significant (P = 0.002). The average distance from the medial femoral head to the teardrop was 13 mm preoperatively (range, 8–16 mm) compared with 11 mm (range, 6–18 mm) postoperatively, which was statistically significant (P = 0.022). The mean radiographic sphericity index improved from 1.29 (range, 1.1–1.6) at the time of frame application to 1.17 (range, 1.0–1.59) at the time of frame removal, which was statistically significant (P = 0.001). The Stulberg classification based on the most recent radiographs was as follows: Class I, one hip; Class II, five hips; Class III, eight hips; and Class IV, four hips (unpublished study).
12.1.5 Complications
Most patients developed minor pin tract infections, which were successfully treated with oral antibiotics. The fixator on one patient had to be removed after only 2 months because of severe pin tract infection. This patient developed recurrent stiffness and subluxation of the hip after the first removal. After the second treatment, the patient was able to maintain a mobile hip with spherical hip motion.
One patient sustained a fractured neck of the femur caused by a fall on the day of fixator removal. The fracture was treated by screw fixation and healed uneventfully.
Two patients each underwent a second application of the fixator for contralateral Perthes disease at 3 years and 3 months and at 1 year and 4 months, respectively, after the index distraction treatment. One patient underwent treatment of Perthes disease shortly after a subchondral fracture of the hip. The course of treatment by distraction was uneventful. However, after fixator removal, the femoral head proceeded to undergo resorption, collapse, and subluxation. Reapplication of the external fixator a year later, during the maximum resorption phase, led to an excellent final result.
As an addendum to this study, I decided to review the radiographs and results of as many patients that could be located in 2009. This represented a 20-year follow-up on the earliest patient. Only 13 of the total hips and 11 of the total patients could be found. All of the Stulberg 4 cases were in the follow-up group. It is interesting to note that all of the Stulberg 4 cases had evidence of degenerative changes, while none of the Stulberg 1, 2, or 3 cases did. Only two of the four Stulberg 4 cases were symptomatic, while the others were not. Femero-acetabular impingement (FAI) was present in all of the Stulberg 3 and 4 cases reviewed. We were unaware of FAI when we first conducted this study. Some of the Stulberg 3 cases are being considered for femoral head reduction osteotomy. The Stulberg grade did not change at final follow-up in 2009. The result grading also did not change since the two painful Stulberg 4 cases were the same symptomatic cases in the original study. It is clear that the four Stulberg 4 cases will all require a hip replacement. It is likely that the Stulberg 3 cases will require some treatment for FAI which could include hip arthroscopy or surgical dislocation of the hip with osteochondroplasty or femoral head reduction osteotomy (Paley 2011).
12.1.6 Discussion
The natural history of Perthes disease and avascular necrosis of the hip joint is directly related to patient age at time of disease onset and amount of femoral head involvement (Gower and Johnston 1971; McAndrew and Weinstein 1984; Yrjonen 1999; Ippolito et al. 1985). Older age and whole femoral head involvement are poor prognostic factors (Ippolito et al. 1987; Norlin et al. 1991; Mazda et al. 1999; Eyre-brook 1936). Treatment by bed rest, non-weight bearing, and abduction orthosis is of limited value and is not well tolerated (Kamhi and MacEwen 1975; Meehan et al. 1992; Eaton 1967; Martinez et al. 1992). Range-of-motion exercises and various forms of surgical containment have constituted the mainstay of treatment for Perthes disease (Lack et al. 1989; Bankes et al. 2000; Klisic 1983) that for children older than 6 years, any method of treatment offers a better prognosis than no treatment. Containment treatment in patients older than 11 years leads to only 40 % satisfactory results (Catterall 1971; Salter and Thompson 1984) compared with an overall age-independent success rate of 70–90 % (Gower and Johnston 1971).
Stiffness, subluxation, and femoral head collapse are considered contraindications to surgical containment treatment. Therefore, the worst cases often are not treatable with containment. Abduction bracing is a nonsurgical containment treatment method. It is fraught with problems of noncompliance, especially in older children, and can lead to hip stiffness unless prescribed in conjunction with aggressive physical therapy (Martinez et al. 1992). Varus femoral osteotomy can achieve the greatest degree of femoral head containment (Lloyd-Roberts et al. 1976). The resulting coxa vara deformity may not remodel and therefore may produce a long-term limp due to abductor muscle dysfunction because the abductor lever arm and muscle tension are altered (Noonan et al. 2001). A pelvic osteotomy alone for containment is more limited in its amount of coverage (Rowe et al. 2006; Lee et al. 2009). All these methods are contraindicated if the hip is stiff, especially if it cannot abduct sufficiently; these hips are suitable for a salvage procedure.
Both varus femoral and pelvic osteotomy methods distort the anatomy and have limited ability to change the shape of an already collapsed femoral head or to reduce subluxation (Lack et al. 1989).
The distraction we describe is not limited by hip stiffness, degree of femoral head deformity, or subluxation. Although distraction is performed with the hip in 15° of abduction, the primary goal is not containment. The epiphyseal cartilage of the femoral head is not primarily damaged from the loss of circulation to the femoral head. Instead, it reacts by proliferating outside the acetabulum, leading to coxa magna and lateral ossification. The cartilage also proliferates medial to the femoral head when the femoral head has migrated laterally and superiorly (Bennett et al. 2002). Proliferation or ossification is not observed superior to the femoral head, where it is in contact with the acetabulum. Because the femoral head cartilage seems to have the potential to grow in the unstressed regions inside and outside the acetabulum, we postulated that if the femoral head were pulled away from the acetabulum and kept there, the epiphyseal cartilage might proliferate into the acetabulum and fill the space created by the previous collapse. The acetabulum would act as a sort of mold for the femoral head. In many ways, this is similar to the theory behind containment. Pulling the femoral head down also would reduce the apparent subluxation of the hip, especially the break in Shenton line. In cases in which collapse has not occurred or has not progressed to maximum, dead bone may be resorbed under the protection of the distractor. If the distractor remains in place long enough, new bone formation can replace removed bone, preventing collapse after fixator removal. Herring (Salter and Thompson 1984) noted that once the lateral pillar has re-ossified, no further collapse is to be expected. Therefore, we chose re-ossification of the lateral pillar as a satisfactory end point for fixator removal.
The radiographic findings obtained during distraction revealed very rapid progression of osteoporosis of the femoral head and neck. The dead bone could readily be distinguished from the live bone by its white sclerotic appearance; the remainder of the femoral head and neck appeared osteoporotic. At approximately 6–8 weeks after surgery, new ossification of the lateral pillar was observed. The lateral pillar was fully reconstituted by 4 months after initiation of the distraction treatment. In children older than 12 years, this took up to 5 months.
Mose (1980) and Stulberg et al. (1981
 Distraction Arthroplasty for Ankle Osteoarthritis
Distraction Arthroplasty for Ankle Osteoarthritis
 Hybrid Lengthening Techniques: Lengthening and Then Nailing (LATN) and Lengthening and Then Plating (LAP)
Hybrid Lengthening Techniques: Lengthening and Then Nailing (LATN) and Lengthening and Then Plating (LAP)
 Lengthening over Nails (LON): Femur and Tibia
Lengthening over Nails (LON): Femur and Tibia
 Pelvic Inlet Reconstruction for Obstruction Associated with Lumbosacral Agenesis Utilizing Distraction Osteogenesis and Circular External Fixation
Pelvic Inlet Reconstruction for Obstruction Associated with Lumbosacral Agenesis Utilizing Distraction Osteogenesis and Circular External Fixation
 Pelvic Support Osteotomy (PSO): Indications, Limits and Complications
Pelvic Support Osteotomy (PSO): Indications, Limits and Complications
 Reconstruction of Segmentary Defects in Chronic Osteomyelitis Using the Combined Technique
Reconstruction of Segmentary Defects in Chronic Osteomyelitis Using the Combined Technique




Related posts:
Distraction Arthroplasty for Ankle Osteoarthritis
Hybrid Lengthening Techniques: Lengthening and Then Nailing (LATN) and Lengthening and Then Plating (LAP)
Lengthening over Nails (LON): Femur and Tibia
Pelvic Inlet Reconstruction for Obstruction Associated with Lumbosacral Agenesis Utilizing Distraction Osteogenesis and Circular External Fixation
Pelvic Support Osteotomy (PSO): Indications, Limits and Complications
Reconstruction of Segmentary Defects in Chronic Osteomyelitis Using the Combined Technique
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
