Key points
- •
Transpalpebral temporal lateral and supraorbital adhesion release.
- •
Browlift.
- •
Transpalpebral corrugator myectomy.
- •
Transpalpebral midface lift.
- •
Muscular suspension canthopexy.
Patient selection
The transpalpebral approach to periorbital rejuvenation is an option where a patient does not require a full face lift, but still has many of the aging signs that are not expected to be addressed by a standard blepharoplasty. Patient selection is oriented by anatomic and functional findings related to the periorbital aging process and individual requirements. This procedure has a long recovery phase and patients cannot expect to resume their social activities until 3–4 weeks after surgery.
In removing upper lid skin excess, brow ptosis may worsen as this procedure creates more tension at this level, pulling it downward. An additional effect of skin resection and weight reduction on the upper eyelid is the relief of frontalis muscle spasm which maintains brow position. A precise diagnosis of the position and shape of the eyebrows as well as its dynamic changes is essential for the appropriate surgical indication and brow stabilization must be achieved to enhance upper blepharoplasty results.
Vertical glabellar rhytids are related to hyperactive corrugator muscles and may still be noticeable after many years of repeated and painful botulinum toxin injection. The lateral brow is also lowered by the transverse head of corrugator and the lateral portion of orbicularis oculi muscle, which in addition to the temporal soft tissues descent contribute to lateral brow ptosis. Patients who, for whatever reason, refuse botulinum toxin therapy, may be candidates for surgical treatment of corrugator muscle hyperactivity, but they must also be made aware of a definitive loss of corrugator muscle function.
Indications
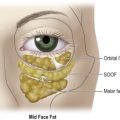
Heavy and ptotic eyebrows, hooded eyelids, and glabellar rhytids with hypertonic corrugator muscles are the most common indications for transblepharoplasty upper face rejuvenation. With the malar pad descent, an infraorbital cheek hollow is present and the contour between the zygomatic eminence and the medial cheek becomes marked as well as the contour between the lateral eyelid and cheek. The depth of the nasolabial fold is also increased. All these manifestations of midface aging are indications for a transpalpebral midface cheek lift.
As most patients present for eyelid surgery, and those who request browlift and upper facial rejuvenation may also require upper blepharoplasty, the upper eyelid incision may be an alternative port to the periorbital zone instead of approaching it from a longer distance with reduced scalp incisions with or without endoscopic assistance, or coronal incision. It may also be performed for full facelift as safely as an endoscopic assisted foreheadplasty ( Figure 11.1 ).




Operative technique
Pre-operative preparation
Markings are done pre-operatively with the head at 45 degrees. The temporal and frontal skin are lifted along the anterior temporal crest to identify the temporal lateral adhesion. A 4 cm scalp incision is marked lateral to the anterior temporal crest 3–4 cm behind the hairline. The redundant upper eyelid skin is marked with the brow elevated to avoid overresection. The patient is asked to frown, contracting the corrugator muscle so that its projection on the superior medial orbital rim is marked. By palpation of the supraorbital rim, the orbital notch is identified and marked as a reference of the supraorbital and supratrochlear neurovascular bundle, usually 2.7 cm and 1.7 cm from the midline.
With the patient under intravenous sedation, the supraorbital and supratrochlear nerves are blocked with a 0.25% bupivacaine with epinephrine 1 : 200 000. An additional anesthetic solution with 1% lidocaine and epinephrine 1 : 200 000 is injected in the upper eyelids and along the superior lateral orbital rim to the lateral canthus. The scalp incisions, the temporal and the frontal area are likewise infiltrated with the more diluted local anesthetic to produce hydrodissection.
Technique
Upward forehead flap elevation
The surgical principles of the transpalpebral subperiosteal approach are the same as those of endoscopic browlift. The only difference is that the surgeon approaches these structures from below and as we are closer to the periorbital anatomical structures, they are addressed first. Initially, determine and outline the area of redundant upper eyelid skin. This should be done after slightly elevating the lateral brow and marking the elevation vectors that will be used during advancement of the forehead flap. When the lateral brow is elevated by advancing the forehead flap, eyebrow skin that has descended onto the orbit is spared from resection. This maneuver will help prevent over-resection of skin in the upper eyelid. After skin is excised, the orbicularis oculi muscle is identified and a 6 cm incision parallel to the skin incision is made to expose the surface of the septum orbitale. Using double hooks the orbicularis oculi muscle is retracted and dissected from the septum in a cephalic direction exposing the superior orbital rim.
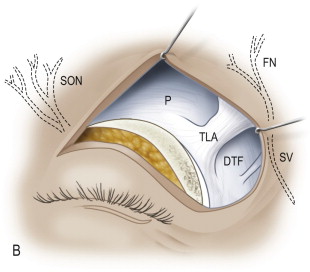
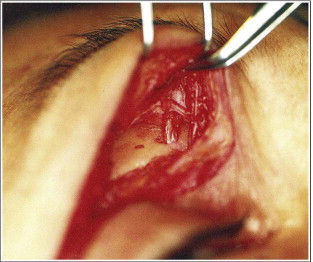
The periosteum is incised 3 mm above the edge of the superior orbital rim, from the upper and lateral limit of the orbit to the exit of the supraorbital neurovascular bundle. Careful dissection will reveal a band of connective tissue between orbital rim and overlying superficial temporal fascial plane near the point where the temporal fusion line meets the superolateral orbital rim. This technique differs from other limited incision techniques as transection of the lateral temporal adhesion (LTA), lateral brow thickening of the periorbital septum (LBT) and lateral orbital thickening of the periorbital septum (LOT) is performed under direct view. The lateral aspect of the dissection allows dissection under direct visualization of the most delicate area of the flap, the lower temporal compartment (LTC) as defined by Mendelson. This compartment contains the sentinel vein, the temporal branch of the facial nerve and the zygomatic nerves. This elevation can be gently performed with gauze leaving these structures above the plane of dissection until the inferior temporal line is reached. With this blunt dissection beyond the lateral limit of the orbit and above the lateral canthus level, the deep temporal fascia is exposed and as the superior and lateral dissection progresses, the sentinel vein will be seen and may be preserved ( Figure 11.2a,b )

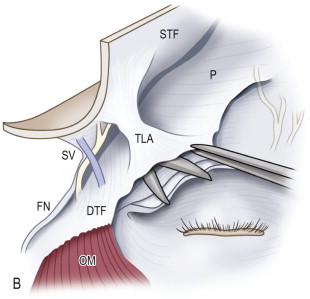
At this level the frontal branches of the facial nerve are in the superficial temporal fascia flap and the lateral temporal adhesion can be safely released connecting the subgaleal fascia with the subperiosteal plane over the frontal bone under direct vision ( Figure 11.3a,b ). The medial aspect of the flap elevation is easier. A periosteal elevator is required to free the zone of firmly fixed soft tissues from bone near the orbital rim. Under direct visualization all the periosteal attachments above the brow are released. Remaining in the subperiosteal plane and stopping its dissection before the supraorbital notch injury to the supraorbital neurovascular bundle is avoided even if it is not visualized. If medial release of the periosteum is necessary, it is safer to do it after corrugator muscle resection and with direct view of the supraorbital and supratrochlear neurovascular bundle ( Figure 11.4 ). The flap elevation should stop approximately 5 cm above the brow (after releasing of the ITL and TLA). Further elevation is subsequently performed through the two scalp temporal incisions.

Scalp temporal incision access
Two scalp incisions are made, the first behind the frontal hairline, almost as high as the lateral segment of a classic coronal incision, and the second perpendicular to the selected suspension vector line. The incision should not be placed more medially than the anterior temporal crest to avoid both injury to the deep branch of the supraorbital nerve and post-operative scalp numbness and dysesthesia. The scalp incisions go through superficial temporal fascia down to the temporalis fascia. There is a clear plane between the temporalis fascia and superficial temporal fascia. After elevating the superficial temporal fascia through the scalp incision, the periosteum is incised at the superior temporal line and elevated in the forehead. Since the inferior region of the forehead has already been released from its deep attachments the periosteal elevation should proceed downwards. At this point the elevation in the frontal region will meet the prior elevation done through the blepharoplasty incisions.
The transpalpebral myectomy of the corrugator muscle
It is advisable to perform subperiosteal dissection in the frontal area before approaching the corrugator muscle to avoid the possibility of excessively stretching the supraorbital neurovascular bundle. The orbicularis muscle is dissected from the anterior surface of the corrugator muscle between its cutaneous insertion and its bony origin. The lateral end of the corrugator muscle is transected just as its fibers pass into the plane of the orbicularis oculi and frontalis muscles. While elevating the lateral end of the transected corrugator supercilii muscle away from the trunk of the supraorbital nerve, the lateral part of the muscle is resected. The supraorbital nerve trunk, before dividing into superficial (medial) containing three or four small branches, and deep (lateral) divisions, is safely deep to the plane of the corrugator supercilii muscle when the soft tissues are retracted away from the orbital rim. However, the supratrochlear nerve branches pass through the anterior surface of the medial third of the muscle and can have four to eight branches.
It is, therefore, recommended to leave a muscle stump interlaced with supratrochlear nerve branches protecting it. This small muscle stump has no effect on glabellar skin. The remaining muscle located medially to the nerve branches is also elevated and resected after total release of its bone origin. This will prevent later recurrence of glabellar action and asymmetry.
The medial head of the orbital portion of the orbicularis oculi muscle and the depressor supercilii are also resected if oblique glabellar skin creases are present. They can be easily identified overlying the origin of the corrugator muscle. Transverse glabellar wrinkles are related to procerus muscle contraction which may also be approached through the eyelid incision, although I prefer to preserve its function and avoid a frozen aspect of the glabella. Moreover, these wrinkles are not usually remarkable and may improve after forehead flap lift.
Fixation
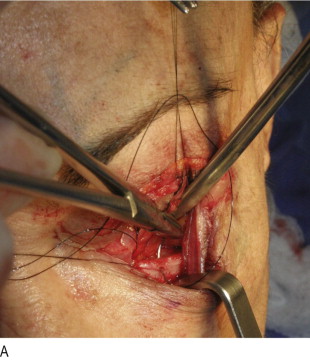
There are many techniques to fix the brow or forehead once it has been elevated off the calvarium in brow elevation procedures. However, fixation was previously accomplished with nylon 2-0 sutures passed through the superficial temporal fascia plane within the margin of the advanced flap and sutured to the deep surface of the temporal fascia of the posterior scalp. Plication and shortening the superficial temporal fascia and pulling the lateral temporal adhesion and the lateral portion of the subperiosteal forehead flap will cause it to reattach at a higher level. An extensive subgaleal and subperiosteal plane will be the healing interface maintaining the elevation of the temple and the forehead. To enhance the flap adhesion to the deep plane in the temporal area, a 2.2 cm window is opened in the deep temporal fascia. The inner surface of the superficial temporal fascia will strongly adhere to the exposed temporal muscle and stabilize the temporal flap at a higher position. Placing a through and through suture in the flap along the temporal line, the forehead and its previously released temporal adhesion is lifted transmitting the pull to the lateral two-thirds of the eyebrow ( Figure 11.5 ). After this fixation, a gap above the orbital periosteum incision exposing the bone surface is often seen through the eyelid incision. Two more sutures are placed at the temporal hairline 1 inch apart and tied to the posterior leaf of the aponeurotic galea, applying enough tension to elevate the temple soft tissues ( Figure 11.6 ). This suspension of the temporal flap will result in excessive scalp around the temporal incision that should not be removed, as it will flatten in 2–3 months without a noticeable scar.
Related posts:
 Anatomy of the upper and lower eyelids
Anatomy of the upper and lower eyelids
 Correction of the tear trough deformity with hyaluronic acid
Correction of the tear trough deformity with hyaluronic acid
 Orbital aging and harmony in orbital rejuvenation
Orbital aging and harmony in orbital rejuvenation
 Midface elevation: one single suture
Midface elevation: one single suture
 Alloplastic augmentation to improve blepharoplasty and midfacial results
Alloplastic augmentation to improve blepharoplasty and midfacial results
 Autogenous, allogeneic and alloplastic lower lid spacers after blepharoplasty
Autogenous, allogeneic and alloplastic lower lid spacers after blepharoplasty
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


