Dermatoscopy
Epiluminescence microscopy (ELM)
Skin surface microscopy
Dermoscopy is an in vivo noninvasive diagnostic technique that magnifies the skin in such a way that color and structure in the epidermis, dermoepidermal junction, and papillary dermis become visible. This color and structure cannot be seen with the naked eye. With training and experience, dermoscopy has been shown to significantly increase the clinical diagnosis of melanocytic, non-melanocytic, benign and malignant skin lesions, with a 10–27% improvement in the diagnosis of melanoma compared to that achieved by clinical examination alone. There is, however, a learning curve to mastering dermoscopy, and it is essential to spend time perfecting it—practice makes perfect!
Technique
In classic dermoscopy, oil or fluid (mineral oil, immersion oil, KY jelly, alcohol, water) is placed over the lesion to be examined. Fluid eliminates surface light reflection and renders the stratum corneum transparent, allowing visualization of subsurface colors and structures. Using handheld dermoscopes that exploit the properties of cross-polarized light (polarized dermoscopy), visualization of deep skin structures can be achieved without the necessity of a liquid interface or direct skin contact with the instrument.
The list of dermoscopy instrumentation is long and continues to grow and evolve with the development of better and more sophisticated handheld instruments and computer systems. Depending on the budget and goals for the evaluation and management of patients with pigmented skin lesions, there is a wide variety of products to choose from.
The 3-point checklist
To encourage clinicians to start using dermoscopy, simplified algorithms for analyzing what is seen with the technique have been developed.
For the novice dermoscopist, the primary goal of dermoscopy is to determine whether a suspicious lesion should be biopsied or excised. The bottom line is that no patient should leave the clinic with an undiagnosed melanoma.
For the general physician, dermoscopy can be used to determine whether a suspicious lesion should be evaluated by a more experienced clinician.
Dermoscopy is not just for dermatologists; any clinician who is interested can master this potentially life-saving technique.
Triage of suspicious pigmented skin lesions
The 3-point checklist was developed specifically for novice dermoscopists with little training to help them not to misdiagnose melanomas while improving their skills.
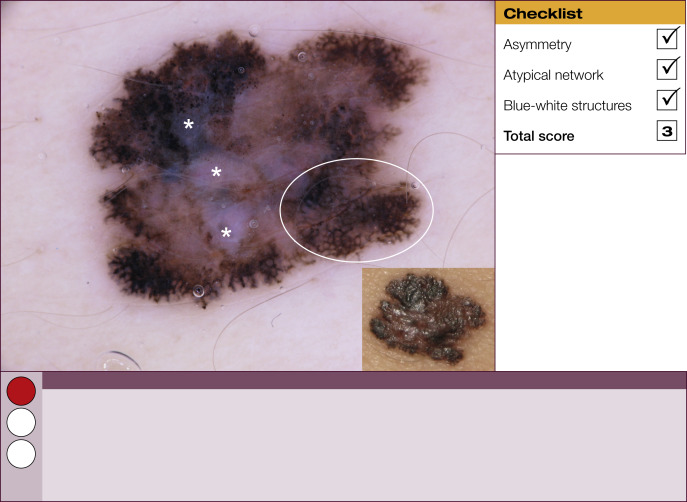
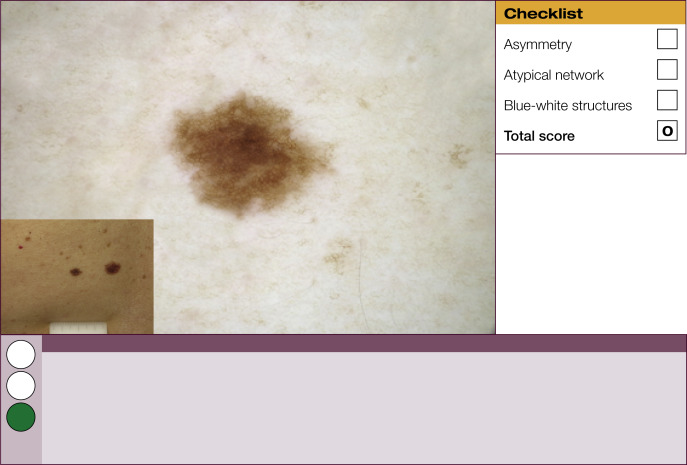
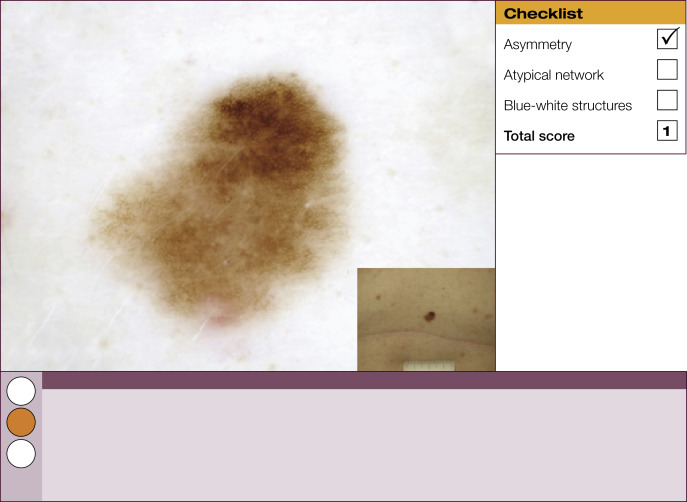
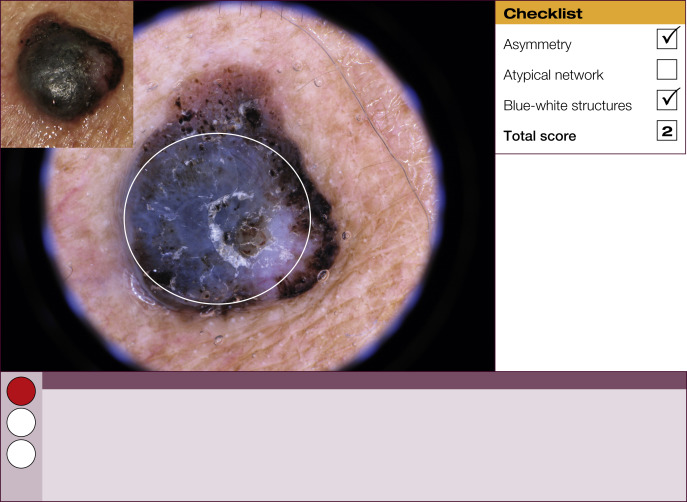
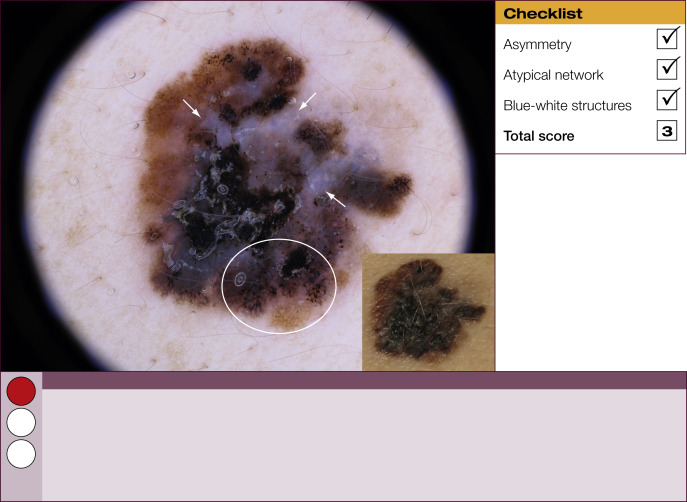
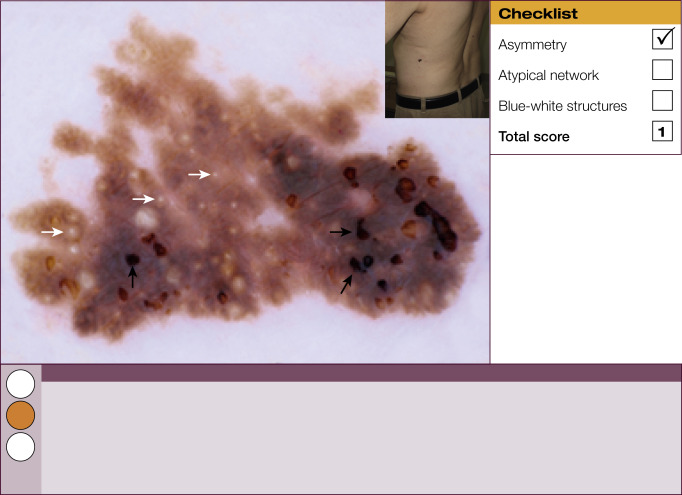
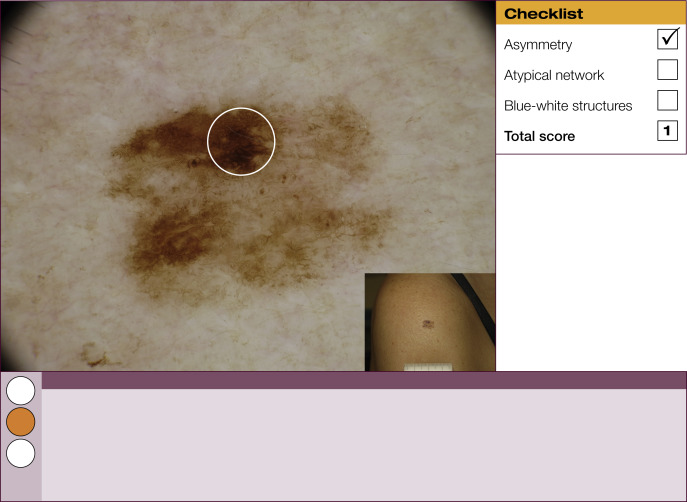
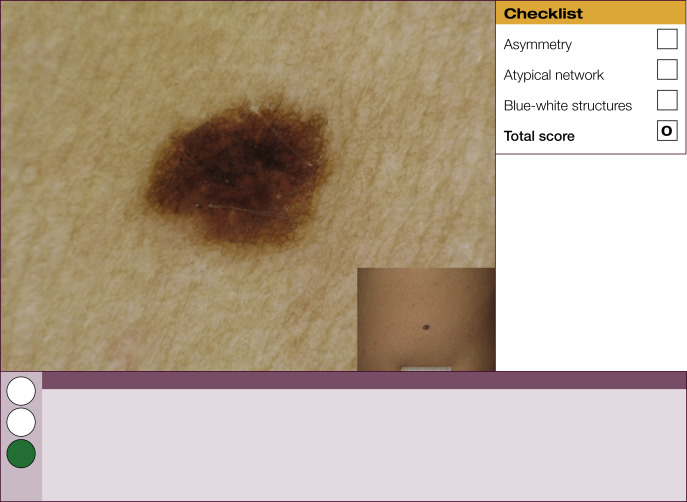
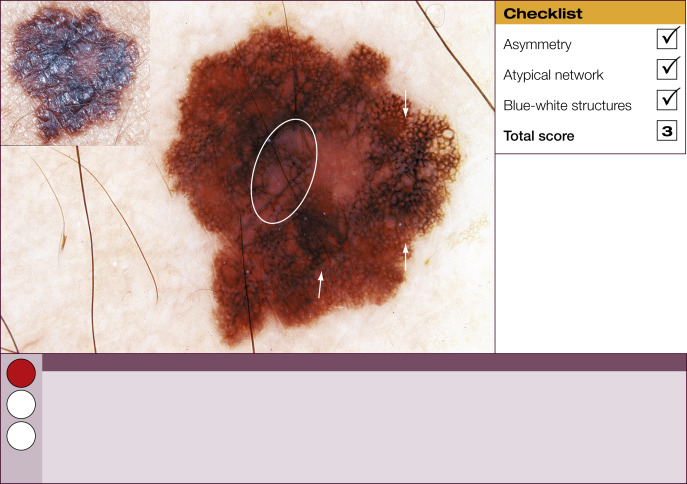
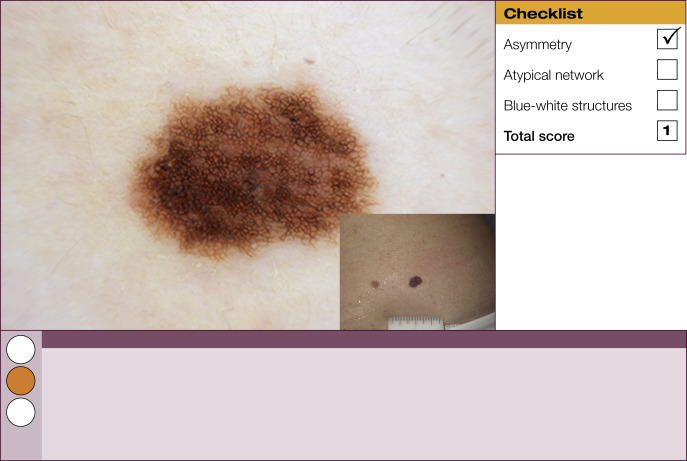
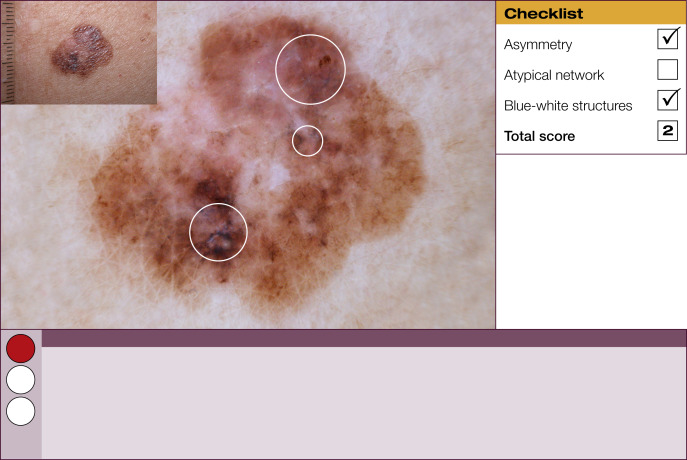
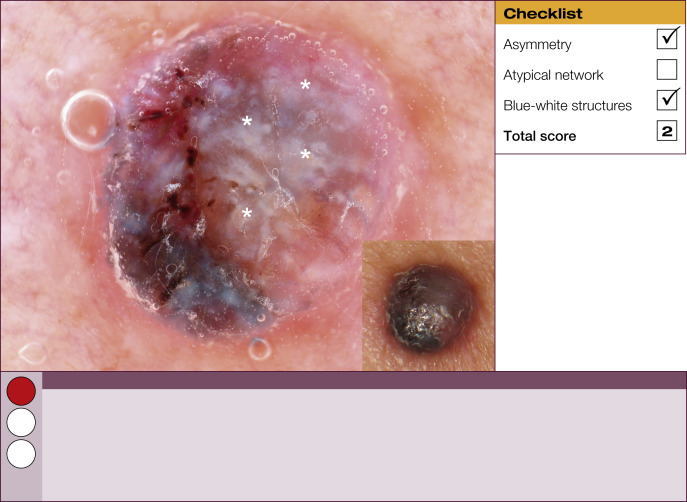
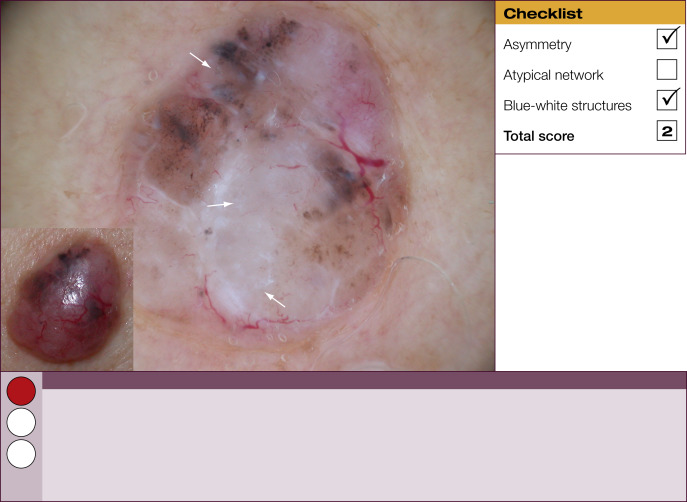
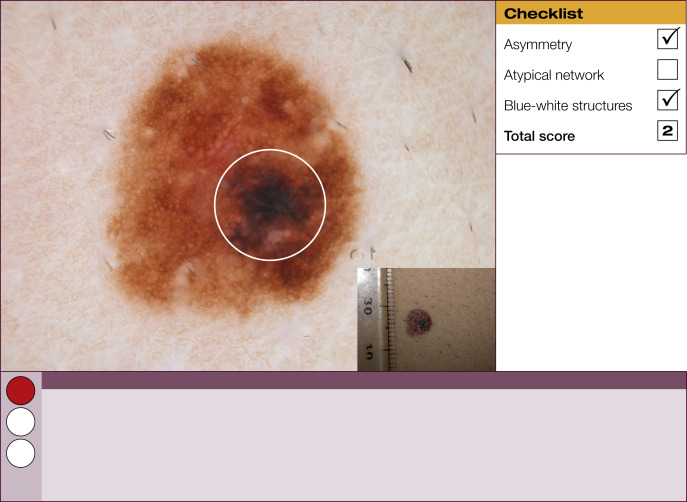
Results of the 2001 Consensus Net Meeting on Dermoscopy (Argenziano G, J Am Acad Dermatol 2003) showed that the following three criteria were especially important in distinguishing melanomas from other benign pigmented skin lesions:
- •
dermoscopic asymmetry of color and structure;
- •
atypical pigment network; and
- •
blue-white structures (a combination of the previous categories of blue-white veil and regression structures).
Statistical analysis showed that the presence of any two of these criteria indicates a high likelihood of melanoma. Using the 3-point checklist, one can have a sensitivity and specificity result comparable with other algorithms requiring much more training. In a preliminary study of 231 clinically equivocal pigmented skin lesions, it was shown that, after a short introduction of 1-h duration, six inexperienced dermoscopists were able to classify 96.3% of melanomas correctly using this method.
This first chapter provides 60 examples of benign and malignant pigmented skin lesions to demonstrate how the 3-point checklist works and the practical value of this simplified diagnostic algorithm.
The 3-point checklist was designed to be used as a screening method. The sensitivity is much higher than the specificity to ensure that melanomas are not misdiagnosed. We recommend that all lesions with a positive test (3-point checklist score of 2 or 3) are excised ( Table 1 ).
| 3-Point checklist | Definition |
|---|---|
| Asymmetry of color and structure in one or two perpendicular axes |
| Pigment network with irregular holes and thick lines |
| Any type of blue and/or white color |


Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


