Internal Mandibular Distraction
Michael Alperovich
Roberto L. Flores
DEFINITION
Mandibular hypoplasia or an underprojected and diminutive mandible can have functional consequences including tongue-based airway obstruction, sleep apnea, reduced intraincisal opening, and malocclusion.1
Mandibular hypoplasia can also result in facial disharmony and distressing aesthetic concerns.2
ANATOMY
The normal mandible can be divided into two, symmetric halves from the midpoint of the mandibular symphysis.
Each hemimandible can be subdivided into several segments: the parasymphysis, body, angle, ramus, and condyle (FIG 1).
The symphysis is the midline of the mandible. The parasymphysis is a region bound by the roots of the mandibular canines. The mandibular body extends from the mandibular canine roots to the mandibular third molar.
The mandibular angle is the triangular region that represents the junction between the mandibular body and ramus. The mandibular ramus is the vertical component of the mandible extending from the angle to the sigmoid notch.
The mandibular condyle is the portion of posterior mandible extending cephalad from the sigmoid notch and articulating with the temporomandibular joint.
The Pruzansky-Kaban classification is widely used to define mandibular deficiency and is most commonly used to classify craniofacial microsomia severity (FIG 2).3
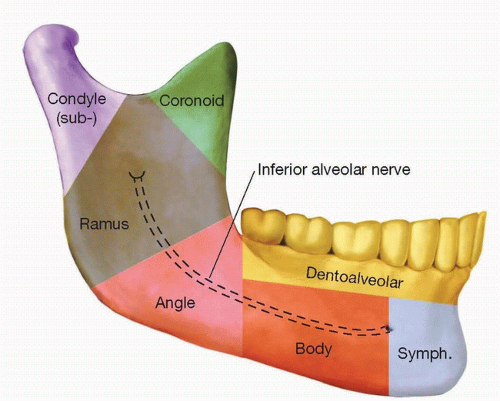
FIG 1 • Schematic demonstrating the anatomic subdivisions of the hemimandible.
A type I mandible features hypoplasia of the mandibular ramus and condyle with a normal mandible morphology.
A type IIA mandible features reduction in the volume of the body, ramus, and condyle but has a preserved temporomandibular joint.
A type IIB mandible features reduction in the volume of the body, ramus, and condyle, as well as medial inclination of the ramus displacing the condyle from the glenoid fossa.
A type III mandible features severe ramus reduction or complete absence with no evidence of a temporomandibular joint.
PATHOGENESIS
Mandibular hypoplasia has congenital and acquired causes, with congenital causes predominating.
Craniofacial microsomia and Pierre Robin sequence are the most common congenital causes followed by Treacher Collins syndrome.4
PATIENT HISTORY AND PHYSICAL FINDINGS
Patients with mandibular hypoplasia secondary to craniofacial microsomia can have malformations in other structures derived from the first and second branchial arches, including the external ear; midface (zygoma and orbit); facial nerve, with the marginal mandibular nerve most commonly affected; muscles of mastication; as well as soft tissue deficiencies.
Unilateral craniofacial microsomia patients will present with asymmetric facies and an upward occlusal cant on the affected side. The ramus is predominantly affected in craniofacial microsomia.
In addition to a hypoplastic mandible, Pierre Robin sequence patients fulfill the triad of micrognathia, glossoptosis, and airway obstruction. Retropositioning of the tongue is responsible for airway obstruction and increased work of breathing. Most patients will also present with a U-shaped cleft palate.
Mandibular hypoplasia in Pierre Robin sequence patients is characterized by bilateral and symmetric mandibular hypoplasia most severely affecting the body.
Up to 50% of Pierre Robin sequence patients have an associated syndrome, with Stickler syndrome as the most common.5
Pierre Robin sequence patients may present with failure to thrive, feeding difficulties, developmental delay, reflux, carbon dioxide retention, heart failure, and desaturations most pronounced in the supine position.
 FIG 2 • Pruzansky-Kaban classification of mandibular deficiency. |
IMAGING
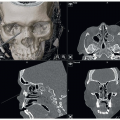
Preoperative imaging should include a craniofacial CT to evaluate mandibular morphology including the TMJ and for planning the ideal vector for mandibular distraction (FIG 3).
A Panorex may be obtained to evaluate occlusion and identify the location of the unerupted tooth buds but is often not necessary if a CT image is obtained.
If applicable, dental study models should be obtained for future orthodontic splint fabrication (ie, correction of any resulting open bite and molding the newly generated bone).
A polysomnogram should be performed to confirm the presence and etiology of sleep apnea.
Bronchoscopy and endoscopy should be performed to identify other potential causes of obstruction.
DIFFERENTIAL DIAGNOSIS
Causes of airway obstruction in addition to retrognathia include the following:
Adenoid/tonsillar hypertrophy
Bronchial stenosis
Bronchomalacia
Central sleep apnea
Laryngomalacia
Subglottic narrowing
Tracheomalacia
NONOPERATIVE MANAGEMENT
There is no nonoperative management for mandibular hypoplasia. Airway compromise associated with retrognathia can be managed through conservative and invasive techniques.
Initial conservative techniques include the following:
Prone positioning
Supplemental oxygen
FIG 3 • Representative craniofacial CT of a patient with Pierre Robin sequence and mandibular body deficiency prior to mandibular distraction.
Nasopharyngeal tubes
Continuous positive airway pressure
Interventional techniques include the following:
Intubation
Tracheostomy
Tongue-lip adhesion
Mandibular distraction osteogenesis
Intubation stabilizes airway management and can be temporizing prior to more definitive approaches.
Tracheostomy will provide a definitive airway; however, the procedure can lead to tracheomalacia, chronic pneumonia, laryngeal stenosis, complex nursing care needs, and impaired psychosocial development.6Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree