The role of hyaluronic acid (HA) fillers in the periocular region continues to expand. In addition to cosmetic uses in the periocular region, HA fillers are increasingly being used to correct eyelid malpositions. This is changing the perspective on the anatomic changes responsible for these malpositions.
Key points
- •
The role of hyaluronic acid (HA) fillers in the periocular region continues to expand.
- •
In addition to cosmetic uses in the periocular region, HA fillers are increasingly being used to correct eyelid malpositions.
- •
This is changing the perspective on the anatomic changes responsible for these malpositions.
Hyaluronic acid (HA) fillers have been in use for many years for cosmetic rejuvenation of the face, specifically for hollows, rhytides, and volume augmentation. More recently, however, fillers have been increasingly used as an alternative to traditional surgical procedures. This article discusses various applications in which fillers are being used beyond the usual cosmetic indications in the periocular region.
One of the most popular uses for HA filler in the periocular region is to treat the tear trough. The tear trough, often referred to by patients as dark circles below the eyes, represents a thinning of the tissues and is bounded by the orbitomalar or orbital retaining ligament. Actually, the hollows around the eye include the tear trough, the temporal inferior orbital rim, the center of the cheek where there may be the “V” deformity, and the superior sulcus. However, the tear trough area seems to draw the most attention from patients.
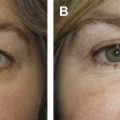
Before the era of fillers, when a patient would present with complaints of lower lid bags, dark circles, or other issues, surgical options were presented that included subtractive blepharoplasty, blepharoplasty with fat repositioning, midface lifting, implants, or any combination of the above. However, fillers offer a nonsurgical alternative in which the bags or dark circles are camouflaged by filling the hollows around them ( Fig. 1 ). This technique produces impressive results that can be achieved during a brief office procedure without the downtime associated with surgery. Moreover, using fillers instead of traditional subtractive or excisional lifting procedures in the lower lid has advanced knowledge of the aging process so that the role of volume loss is better understood.
When performing filler injections to the tear trough region or the orbital hollows, it is important to remember that this area contains the thinnest skin on the face and is the least forgiving. The injections should be performed in the deep preperiosteal plane. Small aliquots are injected slowly as the needle is withdrawn so as not to raise the hydrostatic pressure. The injection can also be carried with a cannula. Lumps and bumps can be very unsightly and may need to be dissolved with hyaluronidase. Also, not every patient is an ideal candidate for filler treatment in this area. The ideal patient will have a relatively short and shallow tear trough, with minimal to moderate fat prolapse, with minimal skin laxity. A less ideal patient will have significant fat prolapse; a deep and long trough or hollow; and thin, lax skin. Filler in these patients can lead to improvement but results may be suboptimal.
To perform a tear trough, lower lid hollow, injection, follow these guidelines:
- •
Slow injection
- •
Stay deep
- •
Preperiosteal
- •
Avoid lumps
- •
Avoid Tyndall
The role of volume augmentation versus lifting has also come into play in the brow region. Many procedures for brow lifting have been described, including but not limited to direct brow lift, internal brow lift, temporal subcutaneous brow lift, endoscopic brow lift, and others. However, there is an element of brow deflation as part of the aging process that may be as significant as perceived brow descent. By reinflating the brow using HA fillers and correcting the volume loss that comes with aging, the brow region can often be rejuvenated without the need for surgical lifting procedures. The HA filler is injected beneath the brow, usually in the temporal region. This corrects volume loss, which often occurs in this area, but will also produce some elevation of the brow ( Fig. 2 ). This may be used in conjunction with neuromodulators. However, fillers to the brow region may also represent an alternative to neuromodulators because there is less chance of creating a brow contour deformity and it provides a more long-lasting effect.
Another area in which HA fillers are playing an increasingly important role is filling the hollow superior sulcus. Most people have a full superior sulcus when they are young. The orbital rim is not visible and the amount of tarsal platform show is usually minimal. An even cursory glance at the latest fashion magazine will show that beautiful models all demonstrate these features of their upper lids, as opposed to a hollowed out superior sulcus with a large amount of tarsal platform show. With age, however, a hollow superior sulcus can develop. There is baring of the superior orbital rim and increased tarsal platform show. This situation can also occur with overaggressive upper blepharoplasty. For many surgeons, the goal of upper blepharoplasty is to remove all of the perceived excess skin, which may not necessarily produce a more youthful appearance.
Before the HA fillers, when a patient presented with a hollow superior sulcus, treatment options included autologous fat transfer, dermis fat grafting, or possible orbital fat repositioning. With the advent of HA fillers, the hollow superior sulcus can be corrected easily in a quick office procedure. When discussing facial rejuvenation, his area is often neglected compared with the lower lid, cheeks, jowls, and neck. By restoring the full lid, eliminating the skeletonization of superior rim, and decreasing tarsal platform show, the aging process is reversed and a youthful appearance restored. This is also an excellent treatment to correct an overaggressive upper blepharoplasty ( Fig. 3 ).