Indications and Techniques for Upper and Lower Blepharoplasty With Microfat Injections
Nuri A. Celik
DEFINITION
Upper Blepharoplasty
Upper blepharoplasty is considered an easy operation; however, depending on your level of expertise and ability to systematically analyze the inherent problems, it might be considered one of the most complex operations of aesthetic surgery practice.
The complex component is the patient evaluation. There is more to a periorbital rejuvenation than just excision of fat, muscle, and skin. We should be able to answer the question: what makes an eye beautiful?
The upper blepharoplasty evaluation should always involve the brow level and shape considerations. Although a high and arched eyebrow is a common feature in female beauty, transverse and low eyebrows are a masculine characteristic in the majority of the male models.
One should always keep in mind that the facial skeleton also plays a major role in the perception of beauty.
A convex area beneath the middle and lateral brow:
A surgeon should always examine the lateral brow mobility before performing an upper blepharoplasty. There are conflicting reports about the brow positional changes following an upper blepharoplasty.1,2 The author has two main criteria for this assessment.
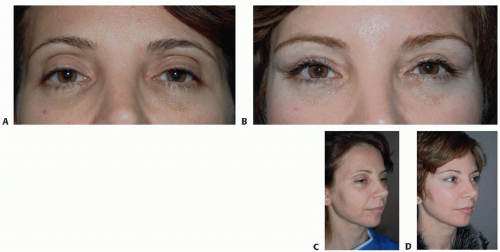
FIG 1 • A,B. A 45-year-old female who underwent upper blepharoplasty and lateral brow lift with fat injection. The levator advancement technique was used to correct the ptosis. C,D. The 2-year postoperative brow contour is achieved with the help of lateral subperiosteal brow lift and fat injection of lateral infrabrow area.
The lateral brow response to a downward pull. This is a sure sign that the skin resection at the end of the upper blepharoplasty procedure will easily displace the lateral brow tissues to a lower position.
Any skin excess lateral to the lateral canthus. This is an indication for a brow lift by the author who never extends the upper blepharoplasty incision beyond the lateral orbital rim, because in thick skin individuals, scars lateral to the rim are visible.
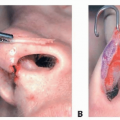
The fullness beneath the lateral brow area is a beauty feature in women3 and can also be a positive factor of masculinity in a low running male eyebrow. The fullness in this area is related to the fullness over the lateral orbital rim, and this can be surgically achieved with fat injection into the area (FIG 1) and also dermofat grafting (FIG 2).
A short supratarsal distance is a significant feature of youth. It is directly associated with the periorbital soft tissue volume and an indicator of the upper sulcus fat content and the levator function.
The skeletonized upper sulcus becomes prominent in the elderly (FIG 3), and the majority of these patients have an increased supratarsal distance. This shows the necessity of the addition of the intraseptal fat management and the levator procedures in our upper blepharoplasty practices.
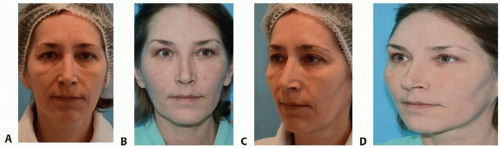
FIG 2 • A,B. A 42-year-old female patient before-after pictures. Upper eyelid ptosis corrected with levator advancement. Notice the raised lateral brow and the fullness of the infrabrow area. C,D. She had lateral brow lift through the upper blepharoplasty incision and dermofat grafting of the upper lateral orbital rim and the upper sulcus. The periorbital contours were obtained with 42-cc fat injection.
The almond shape of the eye aperture:
In young individuals, the medial portion of the eye aperture has a higher measurement vertically than the lateral half.
The better support offered by the lateral canthus during early decades of life provides a higher lateral lower eyelid topography. This decreases the angle of convergence at the lateral corner of the eye and narrows the aperture in the lateral half.
An upper eyelid covering 1 to 2 mm of the limbus:
This is maintained with intact levator function and proper attachment of the aponeurosis on the anterior surface of the upper tarsus.
The upper eyelid level should be evaluated in conjunction with the frontalis muscle activity because the frequent transverse horizontal wrinkles of the elderly show involvement of this muscle as a compensation for the failure of the levator system.
Lateral and medial canthal position and stability:
The effect of the lateral canthal placement and resistance on the position of the lower eyelid is well documented in the literature.
The lateral canthal laxity is not age specific; it might be present in the young (FIG 4A), and surprisingly, the lateral canthus might have good stability in the elderly (FIG 4B).
The medial canthal position and symmetry are also significant factors in the lower eyelid stability because the lower tarsus is attached to both canthi.
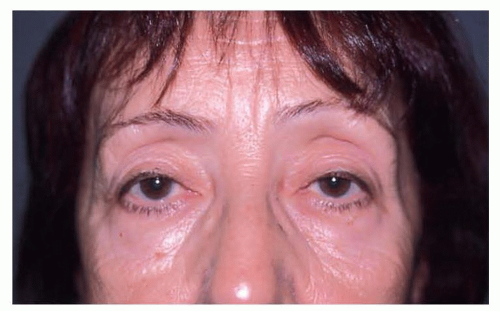
FIG 3 • A 64-year-old female presenting with the typical superior sulcus fat deficiency, ptosis of the upper eyelids, and asymmetrically elevated eyebrows due to frontalis muscle compensation further accentuating the upper eyelid deformity.
Slight asymmetries of the medial canthal origin will alter the hammock-type support of the lower eyelid, interfering with the postoperative results.
The occasional patient who has slight displacement of the medial canthal attachment should be informed preoperatively that the possibility of obtaining perfectly symmetric lower eyelids is compromised (FIG 5).
Medial and lateral canthal laxity is responsible for the majority of postoperative complications and should be taken into account to achieve good results with lower eyelid surgery.
Nasojugal fold:
It is important to obtain a smooth pass from the lower eyelid to the cheek to decrease the shadows that increase with age.
The transformation of the orbital cavity with the aging process decreases the support to the lower lateral orbital rim and the lateral canthus with increased fat herniation and degree of negative factor.6
Lower Blepharoplasty
Lower blepharoplasty is a challenging operation because there are many factors that affect the outcome of surgery. The most important factors are medial and lateral canthal stability, presence of negative vector of the lower orbital rim, and orbital prominence or a shallow orbit.
The need for a concomitant lateral canthal procedure during lower blepharoplasty procedure is not debatable in the author’s opinion.7 It is the author’s experience that patients with a medial canthal attachment at or below the level of the inferior limbus are at increased risk for lower eyelid retraction, no matter what type of maneuver is used for the lateral canthal support.8
Fat Injection
As mentioned before, the telltale sign of periorbital aging is skeletonization; decreased subcutaneous fat fails to camouflage the upper and lower orbital rim bony contours.
With the concomitant brow lift procedures, the relatively thin eyelid skin is pulled superiorly, leaving a depression over the superolateral orbital bony rim.
This area needs augmentation in conjunction with the subbrow area, and the relative prominence of this fill creates a need for temporal hollow, glabellar, and frontal regions and, in select cases, zygomatic arch and midface to be augmented with fat injections.9
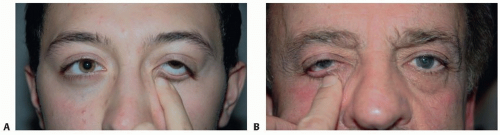 FIG 4 • A. A surprisingly slack lower eyelid in a 24-year-old male patient. Notice the curved contour of the lower eyelid and excessive scleral show for his age. B. A 67-year-old male with good lateral canthal support. |
ANATOMY
The upper eyelid is a complex structure that consists of multiple tissue layers that seem to adhere to each other around the upper anterior tarsal surface.
When the skin and muscle layers are incised and a skin muscle flap is elevated as a superiorly based flap, one notices a thin layer of adipose tissue on top of the upper orbital septum that is more defined medially and somewhat less laterally.
The increased convexity of the globe is possibly responsible for this uneven distribution of the fat layer. The underlying septum should always be incised laterally and higher than the upper tarsal border in order not to injure the levator mechanism inadvertently.
There usually is a preaponeurotic fat pad present, if not previously excised or developmentally absent.
Under the fat pad, toward the upper orbital rim, one can find the vertically oriented fibers of the levator muscle. The surgeon should always keep in mind that, immediately below the levator aponeurosis, there is the vertically oriented arterial loop of the supratarsal arch that might resemble the fibers of the levator muscle.
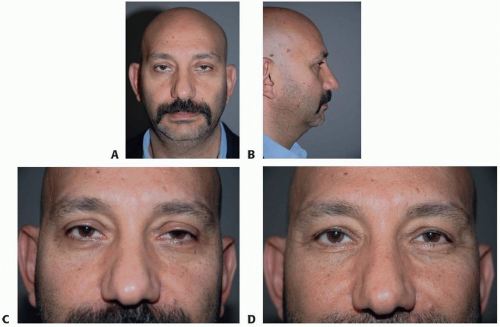
FIG 5 • A,B. A 44-year-old male seeking correction for his asymmetric ptosis, scleral show, and premature facial aging. Notice the low insertion of the medial canthi in relation to the lower limbus. This puts the patient in a “surgical risk” category. C,D. The patient was informed of the asymmetry of his medial canthal insertion and possibility of lower eyelid level and shape mismatch. The postoperative level of the right lower eyelid is slightly lower than the left due to lower insertion of the medial canthus on that side.
The lower eyelid has similar tissue layers converging and attaching to the lower end of the lower tarsus, mainly the septum under the muscle and, in deeper layers, the lower lid retractors and the conjunctiva.
The lower half of the orbital septum is almost always attenuated and the lower eyelid fat pads are herniated in individuals with protruding fat pockets.
One important surgical landmark is the periosteal attachment of the orbicularis oculi muscle that extends around 1 cm along the medial part of the lower orbital rim.9
The middle and lateral portions of the surface of the bony rim periosteum are covered by the SOOF to a variable degree in every individual. This creates two separate surgical dissection layers: around the midportion of the lower orbital rim, the medial part elevation should always be subperiosteal, whereas the more lateral portions allow a supraperiosteal dissection.
PATHOGENESIS
Many complex mechanisms are involved in the aging process with various contributions from different tissue layers presenting as the individual aging patterns seen in different races and skin types.
Camirand’s paper10 deals with mainly the soft tissue changes, whereas recent investigations4,5,6 point to concomitant bony topographical alterations.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree