Hair transplant surgery involves the transfer of hair from an area of anticipated lifelong permanence to an area of alopecia or evolving alopecia.
The principle of donor dominance, for this procedure, was established in 1959 by Dr. Norman Orentreich.
Appropriate patients may include those with male pattern baldness (MPB), female pattern hair loss (FPHL), posttrauma and postsurgical areas of alopecia, as well as some cicatricial alopecias.
Human scalp hairs grow naturally in individual bundles, called follicular units (FUs), composed of clusters of one to four follicles surrounded by layers of concentric collagen fibers.
Follicular unit transplantation (FUT), when performed properly, consistently results in a cosmetic appearance similar to natural scalp hair growth (FIG 1).
The two primary methods of harvesting the donor hair are the strip excision method and follicular unit extraction (FUE).
The ratio of the donor/recipient area has expanded. Though it is 1:1 with large punch grafts, it is 1:2 to 4 with a strip excision and FUT, thus allowing surgeons to cover larger areas of alopecia with a natural appearance and good cosmetic density.
A 1 cm2 section from the donor strip can cover 2 to 4 cm2 of alopecia.
FUE in conjunction with strip harvest has further expanded the donor availability.
When FUE is used as the exclusive method for donor harvest, this decreases the number of relatively permanent scalp hairs that can be transplanted during a patient’s lifetime, because each of the resultant punctuate scars (typically thousands) must be camouflaged by relatively permanent hairs.
Good surgical planning in hair transplant surgery addresses current and future areas of alopecia. This principle is especially important when treating younger patients (because of their long-term donor/recipient area ratios) and those with limited long-term donor hair availability.
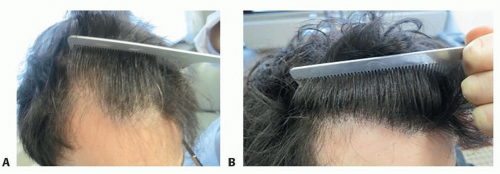
FIG 1 • A. Patient before surgery. B. Results after 1 year.
Preoperative evaluation and determination of candidacy should include a physical exam, review of relevant laboratory tests, and a review of the family history of hair loss.
The scalp is composed of five distinct layers: skin, subcutaneous layer, galea aponeurotica, loose connective tissue, and pericranium.
The scalp has an excellent blood supply provided by a system of anastomoses between branches of the external and internal carotid arteries. The arteries run centripetally within the subcutaneous layer. This rich blood supply helps promote exceptional healing after scalp surgeries (FIG 2A).
The sensory nerve supply is also centripetal and subcutaneous. If larger nerve trunks are injured in surgery, there can be significant hypoesthesia in the postoperative period (FIG 2B).
The anatomy of the hair follicle has been described in many texts. The terminal hair is divided into an upper (infundibulum), middle (isthmus), and lower (inferior segment) region. A good harvest will remove intact follicles, and all segments will be transplanted (FIG 2C).
Androgenetic alopecia
Androgenetic alopecia is the most common cause of hair loss in both men and women. It is also the most common reason for hair transplantation.
In unaffected scalp, the hair has a growing anagen phase of 2 to 6 years, an involution catagen phase of 2 to 3 weeks, and a resting telogen phase of 2 to 3 months.
In affected scalp, the anagen phase is significantly shortened, leading to the production of shorter and finer hairs.
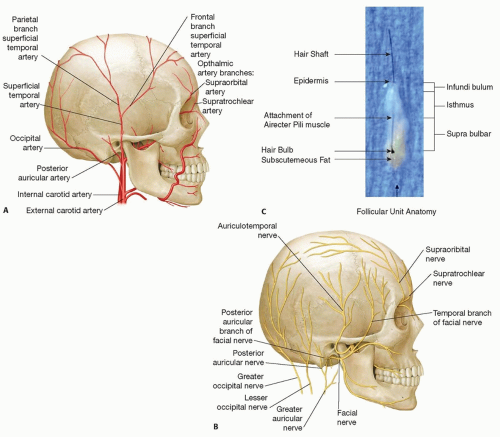
FIG 2 • A. Arterial distribution of the scalp. B. Nerve distribution of the scalp. C. Structure of the hair follicle.
Androgens play a significant role in both MPB and FPHL, although FPHL has a more complex etiology involving multiple other potential sources, including inflammatory reactions and changes in estrogen and other hormone levels and the enzyme aromatase.
Genetic factors are important in determining the likelihood of developing MPB and FPHL—however, it is a polygenic mode of inheritance, with incomplete penetrance.
Cicatricial alopecias
Cicatricial alopecias are, for unknown reasons, increasing in incidence in the population and therefore need to be considered in patients presenting with hair loss. The imposters of patterned hair loss to be wary of include frontal fibrosing alopecia (FFA), lichen planopilaris (LPP), and central centrifugal cicatricial alopecia (CCCA). Their pathogenesis is described in detail in other texts.1
Dermatoscopic exam and biopsy are helpful in diagnosis and evaluation of activity.
Surgery should ideally be avoided until the condition has become quiescent for at least 1 year.2
Patient history should focus on factors that may contribute to hair loss, including symptoms of hypo- or hyperthyroidism, adrenal imbalances, prolactinomas, nutritional deficiencies, and scalp symptoms noted by the patient (burning, itching, tenderness, flaking).2
The history in female patients should also include questions that may indicate symptoms of androgen excess, such as those seen in women with polycystic ovarian syndrome (hirsutism, irregular menses, reproductive challenges, indicators of insulin resistance).4
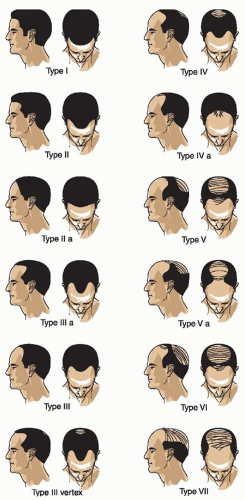
FIG 3 • Norwood classification. (From Landeck L, Otberg N. Hair loss. In: Schalock PC, Hsu JTS, Arndt KE, eds. Lippincott’s Primary Care Dermatology. Philadelphia, PA: Wolters Kluwer; 2010:410-436, with permission.)
Events or conditions that cause telogen effluvium should be ruled out; these most often include major physical or emotional stresses, post-severe febrile illness, postsurgery, and postpregnancy. Hair transplant surgery should not be performed until at least 6 months after the resolution of the effluvium—this allows the donor hair to start regeneration and helps identify major areas of concern.
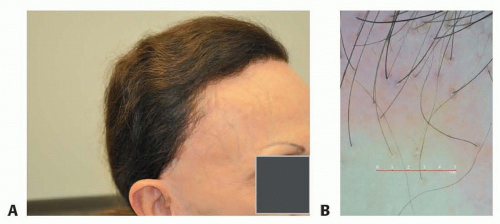
FIG 4 • A. Distribution of hair loss in a patient with frontal fibrosing alopecia (FFA). B. Dermatoscopic photo showing the periphery of FFA. Characteristics include alopecic area devoid of follicular ostia, slightly white in color; hair in the periphery shows perifollicular casts and relative absence of vellus hair.
The history should also clarify the pace of the hair loss and unusual accelerations—a very rapid onset of shedding raises suspicion for etiologies other than androgenetic alopecia.
The family history of hair loss is pertinent as a guide to determine the eventual degree of patterned loss but is not accurately predictive in many patients.
Dermoscopy has become a very useful tool in evaluating patients for hair transplant surgery (FIG 4).
A thorough dermatoscopic exam may reveal more subtle signs of diseases more appropriately treated with a medical rather than surgical approach—including frontal FFA, LPP, CCCA, and alopecia areata patchy or diffuse type.
Dermoscopy can also help to determine the degree of miniaturization in the hair-bearing rim. This may inform the surgeon as to how conservative or aggressive the surgical plan should be.5
Biopsy and dermatopathological evaluation may be useful to confirm the underlying condition responsible for the alopecia. Again, dermoscopy guidance may be helpful in this process to guide the surgeon in the area most appropriate for biopsy.
Patterned hair loss may be difficult to distinguish from these entities, especially in their less active periods.
There also may be some coexistence with MPB/FPHL:
Alopecia areata and diffuse alopecia areata (“incognito”)
Telogen effluvium
FFA
LPP
Tinea capitis
CCCA
Discoid lupus erythematosus
Folliculitis decalvans
Syphilis
Medical therapy
FDA-approved treatments with proven efficacy for MPB include minoxidil and finasteride (FIG 5A,B).
FDA-approved treatment with proven efficacy for FPHL is topical minoxidil 2% twice daily or 5% once daily. Off-label treatments include antiandrogens such as finasteride, spironolactone, and cyproterone acetate.2
Dutasteride 0.5 mg daily may also be used (off-label) in patients who fail to show response to finasteride.
Prostaglandin analogs: Studies thus far have been limited and have failed to show a significant positive effect.

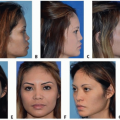
FIG 5 • Male patient before (A) and 1 year after (B) initiating medical treatment with finasteride 1 mg daily. Female patient with typical hair loss in the frontotemporal regions before (C) and 4.5 months after (D) one treatment with PRP/ACell/microroller.
Low-level laser and light devices for hair loss have been shown in limited studies to produce some benefit as compared to sham devices—proposed mechanism of action is mediated by absorption of cytochrome oxidase, resulting in increased oxygen consumption and adenosine 5′-triphosphate (ATP) production. In some patients, it may also produce and anti-inflammatory effect.2
Mesotherapy: Superficial scalp injections of pharmaceuticals and vitamin compounds. Compounds used include minoxidil, biotin, pantethol, finasteride, dutasteride, tretinoin, and other vitamins and minerals. Further studies are necessary to determine efficacy and which compounds at which concentrations are optimal.
Platelet-rich plasma (PRP): Very few controlled studies have been completed to provide evidence-based data on this modality for hair loss treatment. Nevertheless, anecdotal reports and the experience of credible hair restoration surgeons (HRS) are encouraging.6
There are many approaches being used by HRS for this procedure. Standardization is necessary and will enable more meaningful evaluation of the procedure’s efficacy.
Typically in our practice, 60 mL of blood is drawn from the patient and centrifuged to produce PRP. This is then mixed with 25 mg of ACell (an extracellular matrix derived from a porcine bladder) and injected into the area of hair loss. It may be used as a stand-alone procedure or to enhance the results in hair transplant surgery (in the latter scenario, it is also used to bathe grafts prior to implantation).7
When done as a stand-alone procedure for hair loss by one of the authors, microneedling with a 2.5-mm microneedle is performed prior to injection of the PRP/ACell.
PRP has been demonstrated to increase overall hair counts and hair diameter, while microscopic findings reveal thickened epithelium, proliferation of collagen fibers and fibroblasts, as well as greater numbers of blood vessels around hair follicles in areas that have been treated with PRP (FIG 5C,D).7
More studies are needed to confirm the efficacy of this treatment, the ideal approach to be utilized, and frequency of treatments required.
Micropigmentation is a technique that utilizes tattoos to simulate short hairs on the scalp.
It can be used to hide scars and create the illusion of greater hair density in hair-bearing areas. The type of pigment, color chosen, and depth of ink placement can impact the long-term appearance of this type of camouflage.
Other camouflage techniques include
Small hairpieces
Powders or hair fibers that camouflage the color contrast between hair and scalp, thereby making hair appear fuller
Alternative hair styling
Donor area evaluation is undertaken to determine the area from which hair is most likely to be permanent and thus will ostensibly persist in the recipient area long after transplantation.
The senior author conducted a study of 328 men aged 65 years or older in whom areas containing at least 8 hairs per 4-mm diameter circle were measured.3 The dimensions established from this study represent the region of harvest that would be “safe” (ie, the hairs would persist) in approximately 80% of patients under the age of 80 years. This persisting region of the donor scalp was termed the “safe” donor area (SDA) and later the safest donor area to denote that no area is perfectly “safe” (FIG 6A).
These boundaries have since been modified for FUE. Because of the less visible resultant punctate scarring from this alternative technique, Cole’s FUE SDA is somewhat expanded (203 cm2) and includes 14 subdivisions based on hair density but importantly was based on only 94 patients, nearly all of whom were in their 30s or 40s—and for both reasons, it is therefore most probably a less reliable guide regarding long-term planning (FIG 6B).
Donor harvest approach
As previously mentioned, there are two main donor harvest approaches: strip harvest and FUE.
TABLE 1 summarizes the benefits and disadvantages of each method.
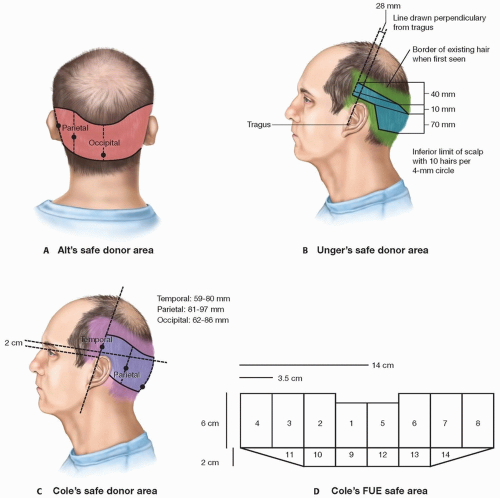
FIG 6 • Unger and Cole safe donor area.
Table 1 Benefits and Disadvantages of Follicular Harvest Techniques
Method
Pros
Cons
Strip harvest
Higher FU yield
Narrow donor area
Higher follicle survival
More protective tissue surrounding hair follicles and predictable graft quality
Harvest stays within the confines of the safe donor area
Ability to choose the size of the grafts
Donor not visible under hair from day 1 postop
Long linear scar that may be visible when the hair is cut short
More painful postop period
Longer postop healing period with some exercise restriction
Potential for loss of dormant follicles—greater in unrecognized cases of telogen effluvium
FUE
Shorter postop healing
Less painful postop period
Minute punctuate scars that are less visible even with the hair worn short especially with less contrast between hair and scalp color
A good complement technique when scalp laxity is limited or for repairs
Less tissue discarded with potential dormant follicles
Lesser FU yield
Wider donor area harvested (some HRS extend past the safe donor area to achieve higher graft yield)
Less tissue around hair follicles (skinny grafts) and less predictable quality, contributing to lower follicle survival
Usually requires shaving the donor area for larger sessions
Lowers the density in the donor area perceptibly after larger harvests or multiple procedures
Ideally, HRS should have all tools available to tailor the procedure to each patient’s individual needs.
Both methods of harvest primarily use follicular unit (FU) grafts almost exclusively in the recipient area.
One of the authors sometimes uses double follicular units (DFU) when a strip harvest is use and the area to be treated has pre-existing permanent hair. This very frequently pertains to women with thinning behind the hairline zone and older males with minimal hair/skin color contrast.
Donor strip harvest
Goals
Minimize the amount of hair follicle transection as the strip is excised and dissected.
Extract donor strip widths with prudent caution in order to minimize closing tension.
Produce only a single scar regardless of the number of sessions performed on a single patient.
Assessment of scalp laxity prior to surgery is of tantamount importance; this can be done with calipers or manually.
The donor strip should be removed from the densest zone of the fringe hair. Any subsequent strip excision should include the previous scar so only one thin linear scar remains.
FUE
Goals
Maximize the amount of hair removed from the most permanent hair-bearing fringe while minimally altering the architecture of the donor area. Keep in mind also that the fringe hair will continue to decrease in density somewhat over the patient’s lifetime.
Minimize transection during extraction, yet try to harvest with some protective tissue; this should be a goal even if the technique involves fractional harvesting of follicular groups.
Minimize the amount of scar tissue within the donor area by varying punch diameters to keep it as small as possible (without increasing transection rates) and try to evenly disperse the harvest sites.
FUE grafts may be removed from the Unger’s traditional SDA and should ideally have a tapering zone superior and inferior to make the density change more subtle. The temporal regions may also be harvested more extensively with this technique than with strip harvesting.
FUE may be used to harvest hairs from the beard area on the neck and inferior to the lower mandible.3 These grafts can be used to camouflage scars and to thicken regions that already have been transplanted. Other body hair survival is much more unpredictable.
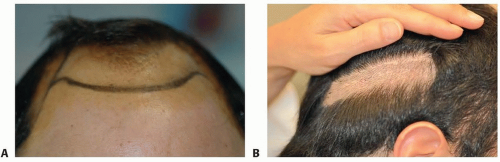
FIG 7 • A. Markings for hairline and borders for surgery. B. Preoperative period after donor area hair has been trimmed. A scar from the previous surgery is visible in the center of the trimmed region.
Recipient area approach
The authors strongly believe in planning that includes treating current areas of hair loss simultaneously with future areas of loss in the zone of the recipient area being addressed (front, midscalp, or vertex).Related posts:
 Injection of Botulinum Toxin to the Depressor Anguli Oris
Injection of Botulinum Toxin to the Depressor Anguli Oris
 Technique for Ptosis Correction
Technique for Ptosis Correction
 Indications and Techniques for Fat Grafting for Periorbital Rejuvenation
Indications and Techniques for Fat Grafting for Periorbital Rejuvenation
 Indications and Techniques for Short-Scar Face-Lift
Indications and Techniques for Short-Scar Face-Lift
 Technique for Ethnic Rhinoplasty Using the Open Approach
Technique for Ethnic Rhinoplasty Using the Open Approach
 Indication and Technique for Diced Cartilage and Fascia Grafting in Rhinoplasty
Indication and Technique for Diced Cartilage and Fascia Grafting in Rhinoplasty

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


