Indications and Techniques for Bridge of Bone Canthopexy
Dev Vibhakar
Erez Dayan
Michael J. Yaremchuk
DEFINITION
The positions of the lateral canthi are important functional and aesthetic facial landmarks. Their position is a fundamental determinant of the shape of the palpebral fissure.1
The terminology of lateral canthal surgery may be confusing. A lateral canthopexy repositions the lateral canthal mechanism without violating the commissure. Canthoplasty procedures, by design, alter the shape of the palpebral fissure, because they disassemble and reassemble the lateral commissure while often shortening the lower lid margin.2,3
Bridge of bone lateral canthopexy requires exposure of the lateral orbit and mobilization of the lateral canthus soft tissue mechanism. Its efficacy is based on the stable suture fixation point provided by drill holes placed relative to the zygomaticofrontal suture in the bone of the lateral orbit. It is our preferred technique for most surgical indications.
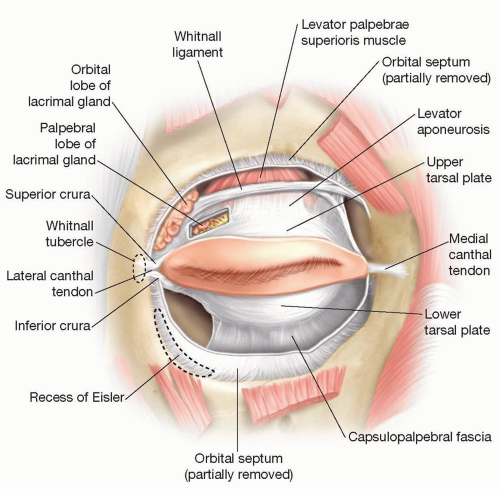 FIG 1 • Position of the medial and lateral canthal ligaments with respect to the bony orbit, tarsal plates, and underlying ligamentous structures |
ANATOMY
The lateral canthus is more correctly termed a lateral retinaculum. The retinaculum receives contributions from the lateral horn of the levator aponeurosis, the lateral extension of the preseptal and pretarsal orbicularis oculi muscle (lateral canthal tendon), the inferior suspensory ligament of the globe (Lockwood ligament), and the check ligament of the lateral rectus muscle. It has a broad attachment to the periosteum over the Whitnall tubercle (FIG 1).4
Variations of the point of attachment or length of the retinaculum will alter eyelid shape, tension, and contour.5
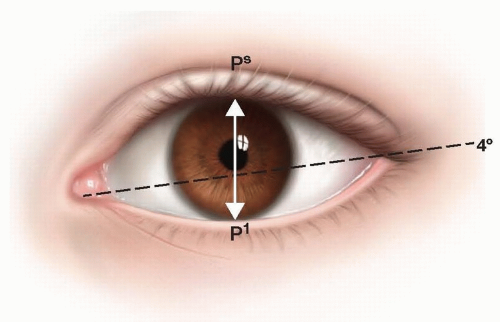 FIG 2 • Dimensions of the palpebral fissure measured in young Caucasian women. The mean height of the palpebral fissure measured from the upper lid (Ps) to lower lid (Pi) margin at the midpupil was 10.8 ± 1.2 mm (n = 200). The mean length of the eye fissure measured from medial commissure to lateral commissure was 30.7 ± 1.2 mm (n = 200). The mean inclination of the eye fissure was 4.1 ± 2.2 degrees. |
PATHOGENESIS
Medial and inferior canthal malposition changes the width and shape of the palpebral fissure as well as the position of lower eyelid resulting in the round eye deformity.1
Inferior displacement of the lower eyelid may cause lagophthalmos leading to inadequate globe protection and exposure keratitis. Epiphora secondary to a displaced lower punctum and impaired tear drainage may also occur.
The etiology of canthal malposition may be hereditary, senile, paralytic, traumatic, or iatrogenic.4
PATIENT HISTORY AND PHYSICAL FINDINGS
History and physical examination are the most important elements of preoperative assessment and planning for both reconstructive and cosmetic procedures. Standard preoperative photographs are taken and reviewed with the patient.
History of recent eye surgery, dry eye, or visual acuity changes should be specifically elicited.
Physical examination findings for lower eyelid malposition include canthal tilt, lid snapback test, lid distraction test, vector analysis, scleral show, and the presence of chemosis or keratoconjunctivitis. Other patient-directed examination includes visual acuity testing, Schirmer test for lacrimation, and slit-lamp evaluation.
IMAGING
Whereas preoperative radiologic examination is uncommon for purely aesthetic surgery, computerized tomographic (CT) evaluation is almost routine for reconstructive procedures. CT scans provide the ability to view anatomic features in different planes and in three dimensions.
SURGICAL MANAGEMENT
Preoperative Planning
Informed consent should include intrinsic risk of canthal malposition and potential for temporary postoperative chemosis.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree