Indications and Technique for Fat Grafting for Periorbital Rejuvenation
Dino Elyassnia
Timothy Marten
DEFINITION
The hallmark of a youthful, attractive orbit is fullness. It has become clear that fat atrophy is a significant component of periorbital aging that results in volume loss and a hollow appearance around the eyes.
Traditional blepharoplasty procedures have focused on treating skin laxity, fat herniation, canthal laxity, and levator dehiscence but have largely ignored fat atrophy. Often, blepharoplasty procedures aggressively remove fat from the eyelids, further compounding the problem of volume loss.
Periorbital fat grafting represents a new paradigm in eyelid aesthetics that focuses on volumetric rejuvenation of the upper and lower eyelids. This approach produces a full, healthy appearance to the eyes that has not been possible with traditional blepharoplasty techniques.
ANATOMY
In recent years, a great amount of work has been done to beautifully elucidate the detailed fat compartments of the face.1
Although this work has been a great contribution to further understanding of facial anatomy, it plays a smaller role in technically carrying out periorbital fat grafting because the goal is not to inject fat in such a way that we aim to “refill” each deflated fat compartment.
PATIENT HISTORY AND PHYSICAL FINDINGS
A focused history should include any ophthalmologic conditions, previous blepharoplasties, or other aesthetic treatments including filler use. As hyaluronic acid filler tends to last especially long in the upper and lower eyelids, knowledge of its use must be obtained so a decision can be made whether to dissolve the material prior to fat grafting.
Physical exam of the eyelids should include looking for the presence of ptosis, dermatochalasis, lower lid fat herniation, canthal laxity, orbital vector, and degree of fat atrophy of the eyelids, midface, and cheek. If problems other than fat atrophy are present such as significant lower lid fat herniation or excess skin, traditional blepharoplasty techniques may need to be combined with fat grafting.
A significant advantage of periorbital fat grafting over traditional lower lid blepharoplasty is that fat grafting is very safe in the setting of dry eye or the presence of canthal laxity, whereas these problems represent relative contraindications for lower blepharoplasty.
Regarding fat harvest, thin patients should be examined at the time of their consultation because patients with limited fat stores often present significant challenges. Extra time and effort will be required to obtain fat from them. Anesthesia and OR times must be calculated accordingly.
Although the abdomen is often cited as the “best” and most convenient site for fat harvest, in our practice, the hip, waist, and outer thigh are the harvest sites of choice. The abdomen typically has thinner, less forgiving skin than the hip, waist, and outer thigh (especially in the face-lift age group) and is readily open to detailed inspection by the patient after the procedure. As such, it can be problematic as a sole donor site in many cases if more than a small amount of fat is needed. The hip, waist, and outer thigh taken together by contrast typically provide more volume and are less subject to surface irregularities, and fat harvest from these areas generally provides more overall improvement in the patient’s silhouette.
IMAGING
Typically, radiographs are not necessary for periorbital fat grafting.
All patients should have standardized photographs taken preoperatively, and any markings made preoperatively on patients should be photographed as well.
These photos should be used intraoperatively to help guide precise placement of fat injections.
NONOPERATIVE MANAGEMENT
Fillers to the periorbital area are a viable alternative to fat grafting and have helped patients understand how volume loss contributes to the periorbital and facial aging process.
Advantages of fillers are they have minimal downtime, they are easily adjustable, they can be reversed (if hyaluronic acid is used), and they last particularly long in the periorbital area compared to other regions of the face.
Disadvantages are they require ongoing maintenance; they are time-consuming, painful, and expensive; and they can look unnatural requiring a high level of precision during injection.
SURGICAL MANAGEMENT
Whether the result of illness, aging, or previous overzealous surgical treatment, filling the hollow upper orbit can produce a remarkable rejuvenation of the upper eyelid and eliminate an unnaturally hollow and elderly appearance sometimes referred to by patients as “nursing home” or “owl” eyes (FIG 1).
Like the upper orbit, fat grafting the infraorbital area allows comprehensive correction of age-associated hollowness that lends the face an ill or haggard appearance, “shortens” the
apparent length of the lower eyelid, and produces a youthful, attractive, and highly desirable smooth transition from the lower eyelid to the cheek. This effect is generally unobtainable by traditional lower eyelid surgery, fat transpositions, “septal resets,” midface lifts, free fat grafts, and other like means (FIG 2).
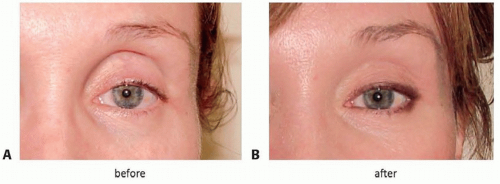
FIG 1 • Correcting upper orbital hollowing. A. Patient with an unnaturally hollow upper eyelid appearance (“owl eyes”) following blepharoplasty performed by an unknown surgeon. B. Same patient seen after fat injections to the upper orbit. A healthier, more youthful appearance can be seen (procedure performed by Timothy Marten, MD, FACS—Courtesy of Marten Clinic of Plastic Surgery).
Although the primary goal of fat harvest is to obtain the “best” tissue for the fat grafting procedure, fat harvesting should be thought of as an opportunity to improve the patient’s figure. Thus, harvest must be undertaken in a thoughtful and artistic manner and generally in a bilateral and symmetrical fashion. Although any area can theoretically be used for a donor site, the hip, waist, and outer thigh are our primary choice for the reasons detailed above.
Preoperative Planning
Fat grafting cannot be performed casually, and deficient areas and key landmarks must be marked preoperatively with the patient in an upright position. Marking will require concentration and focus and is best carried out in an area that is free from distractions.
Creating a proposed plan on a full-page laser print of the patient’s face is helpful in organizing the treatment plan and facilitates confirming with the patient the areas that will be treated.
If the patient wishes, marks can be made while she or he holds a hand mirror. Once markings are complete, a new series of photographs are taken and printed up for use during the procedure. These photographs typically provide the best information to the surgeon intraoperatively.
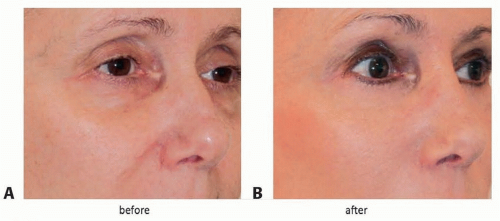
FIG 2 • Filling the hollow lower orbit with fat. A. Patient with an unnaturally hollow and elderly infraorbital appearance. The lower eyelid appears “long,” and there is a distinct line of demarcation between the lower eyelid and the cheek. B. Same patient seen after face-lift and fat injections to the infraorbital area. There is a smooth transition from the lower eyelid to the cheek, and the patient has a healthier, youthful, and attractive appearance (note: the upper orbit, radix, cheek, and nasolabial crease have also been treated with fat injections, and the patient has undergone ptosis correction) (procedure performed by Timothy Marten, MD, FACS—Courtesy of Marten Clinic of Plastic Surgery).
Regarding fat harvest, an estimate should be made as to the amount of fat that will be used and thus the amount that needs to be harvested. In estimating the amount that one needs to harvest, a helpful guideline is that after centrifugation, approximately 50% of what was harvested will be obtained as usable processed fat.
If one wishes to perform the fat grafting procedure predominantly with “stem cell”-rich fat (the bottom 2 cc of fat in the centrifuged 10-cc syringe consisting of high-density adipocytes), only 20% of what is harvested fat will be available for injection, and the total amount harvested will have to be adjusted accordingly.
As in the case of formal liposuction, the patient’s torso must be marked preoperatively while she or he is standing if optimal contours are to be created and if irregularities are to be avoided at the harvest sites. Once markings are complete, marked areas should be photographed and the photos printed up for use during the harvesting part of the procedure.
Positioning
Fat is harvested after anesthesia is initiated but before prep and drape of the face. A complete prep of the torso is not necessary, and in all but the unusual case, a limited prep of the marked area is made and a sterile field is established.
If fat is to be harvested from the hip or lateral thigh, the patient is turned into a semilateral decubitus position; prep, drape and harvest is performed; and the patient then is turned to the opposite side where a similar procedure is performed.
This position can be used to simultaneously harvest fat from multiple sites including the hip, waist, flank, upper buttocks, outer and inner thigh, and knees (FIG 3). With practice, a
well-organized OR team can complete this process expeditiously without undue delay of the procedure.

FIG 3 • Positioning patient for fat harvest. If the patient is carefully positioned in a semilateral decubitus position, fat can be simultaneously harvested from multiple sites including the hip waist, flank, inner knee, outer and inner thighs, buttocks, and inner knee. Obtaining fat from multiple sites is particularly important in thin patients with minimal fat stores or when multiple site fat grafting is being performed. Following harvest from one side, the patient is turned to the other where a similar harvest is performed.
The patient is then returned to the supine position for fat grafting the periorbital area.
Approach
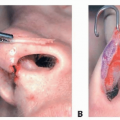
For upper orbit fat grafting, small stab incisions are made in the brow with a no. 11 blade scalpel or a 20-gauge needle. These incisions are so small that they will not require suturing upon completion of the procedure.
Injecting from two separate injection sites at the medial and lateral ends of the brow allows “crisscrossing” of cannula passes during graft placement parallel to the superior orbital rim.
This “crisscrossing” provides smoother fat infiltration and helps avert a “row of corn” effect that may result if injection is made from only one site.
Unlike the upper orbit, however, experience has shown that for the lower orbit, fat is best and most easily injected perpendicular to the infraorbital rim from stab incisions in the midcheek or perioral area. When this is done, lumps and irregularities are far less common. Fat should not be injected parallel to the lid-cheek junction in the infraorbital area.
TECHNIQUES
▪ Fat Harvest
Areas from which fat is to be harvested are infiltrated with a dilute 0.1% lidocaine with 1:1 000 000 epinephrine solution using a multiholed infiltration cannula (TECH FIG 1), and an adequate time is allowed for a proper anesthetic and hemostatic effect.
Approximately 1 cc of this solution is injected for every 3 cc of anticipated fat removal. It is not necessary or desirable to infiltrate in a “tumescent” fashion as overwetting the tissue will result in an overdilute harvest and more time spent in the harvesting process.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree