Fig. 20.1
(a) The standard immunocryosurgery cycle consists of daily application of imiquimod and a cryosurgery session at the end of the second week. Imiquimod is continued for additional 3 weeks, i.e., 5 weeks in total. (b) For benign or premalignant lesions, like genital warts or actinic keratoses, imiquimod is applied every other day, the day prior to cryosurgery and at the same day. Days of imiquimod applications are highlighted with blue color, days off with white
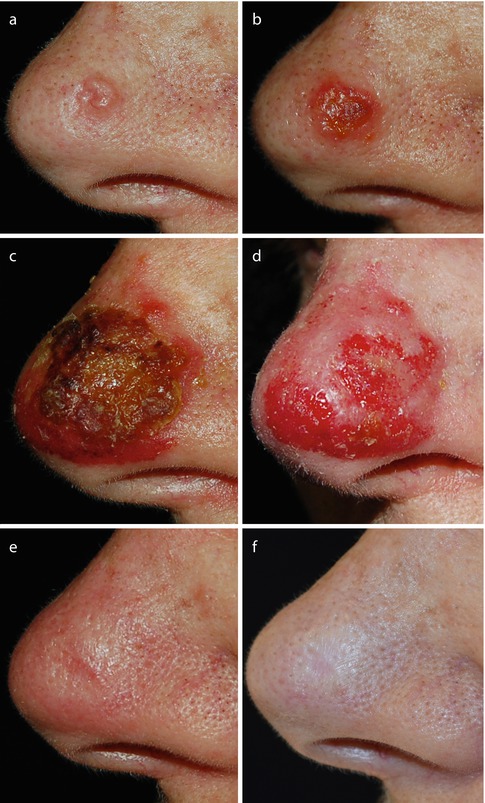
Fig. 20.2
A typical immunocryosurgery cycle treatment in a 75-year-old female patient with a 7 mm basal cell carcinoma on her nose. (a) Baseline. (b) Day 14, after once daily imiquimod application for 2 weeks and prior to the cryosurgery session (liquid N2, open spray, 2 freeze-thaw cycles, 15 s each). (c) Day 35. End of the 5-week treatment cycle. Extensive scabbing is evident. (d) The patient after removal of the scabs. No tumor remnants can be seen and healing is evident (“complete response”). (e) The patient at 3 months follow-up. (f) The patient at 12 months follow-up. The “tumor ghost,” i.e., the skin area that the tumor was infiltrating is evident as a whitish, just perceived scar
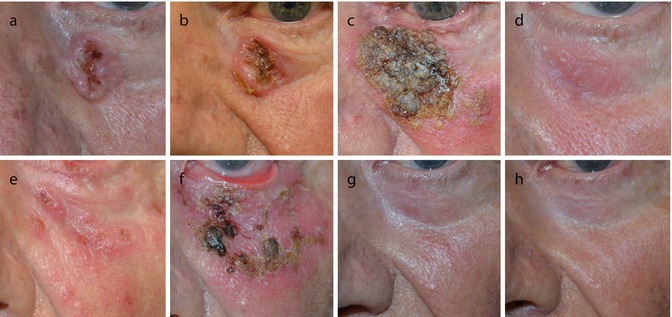
Fig. 20.3
Immunocryosurgery in a large, 17 mm, periocular basal cell carcinoma. (a) The tumor at baseline. (b) Day 14 of the treatment cycle prior to cryosurgery session (liquid N2, open spray, 2 freeze-thaw cycles, 15 s each). Please note relatively minimal inflammatory reaction after 2 weeks once daily imiquimod application. (c) Day 35. After the cryosurgery session the degree of inflammation was intensified and scabbing is evident. (d) 1 month follow-up. Residual tumor is clinically evident and confirmed by biopsy (“partial response”). (e) The immunocryosurgery cycle is repeated, and the patient returns after applying imiquimod for 14 days. (f) Day 35 of the second cycle: end of treatment. A moderate ectropion is evident; there are no clinical signs of rest tumor (“complete response”); (g) 3 months follow-up. The tumor has not relapsed and the ectropion has subsided. (h) 12 months follow-up. The tumor has not recurred; no functional sequelae can be observed

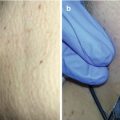
Fig. 20.4
Immunocryosurgery in Bowen’s disease of the skin. (a) The tumor at baseline; (b) Day 14 prior to cryosurgery session (liquid N2, open spray, 2 freeze-thaw cycles, 15 s each). (c) Day 35, end of treatment. (d) One month follow-up. A depressed scar is observed. (e, f) 12 and 36 months after the end of treatment respectively. The scar has improved and is only slightly obvious
There are no specific contraindications for immunocryosurgery; if any, these would be the same as those of cryosurgery and imiquimod. Regarding the known relative contraindications of cryosurgery and imiquimod, we have successfully applied immunocryosurgery to patients under immunosuppressive treatment for either collagen or autoimmune diseases as well as patients with internal, including hematological malignancies and solid organ transplant recipients under immunosuppression without any excess adverse effects attributed to their comorbidities and/or medications. The recommendation in the case of a patient with one of the cold precipitated conditions (Chap. 21) should always balance the benefit over the risk of side effects considering the rather mild cryosurgery session which is required for immunocryosurgery.
The side effects of immunocryosurgery present as an aggravation of the side effects of the treatment with either cryosurgery (Chap. 21) or imiquimod [7] and can be divided into acute ones, seen during the treatment, and late ones. From the acute side effects, the major one is the occasional hefty skin inflammation that characteristically peaks the week after cryosurgery. In some cases of exceptionally intense inflammatory responses, flaring up of susceptible skin lesions in rather remote, not directly treated, sites can be observed. Furthermore, in case the tumor is located in the forehead, ears, or around the eyes, the treatment may elicit pain and headache and significant skin and soft-tissue edema. This is more probable to emerge around the middle of the treatment cycle, and in general it progressively subsides towards the end of the treatment cycle, along with the skin inflammation. In a few cases the patient may experience a flu-like syndrome, particularly in the middle of the treatment, i.e., the week after cryosurgery. Almost all patients report tiredness and anorexia that gradually diminishes by the end of treatment.
At the treated sites, hyper- or hypopigmentation may develop, which improves gradually over time. In many cases, a shallow scar is left behind after successful treatment, corresponding to the skin area involved by the growing tumor before treatment (“tumor ghost”). However, the aesthetic outcome is rated as “good” to “excellent” by both patient and physician, for the latter is also compared to that anticipated after surgical treatment. In few patients, a tingling sensation may persist in the treated area for several months after treatment, sometimes with neuropathic character, which however does not interfere with their daily activities [4, 8]. After treatment, the follow-up plan for continuing care is adapted to the initial diagnosis.
The advantages of immunocryosurgery include low cost, easiness of application in the outpatient setting, high efficacy in the indications used, and excellent cosmetic outcome. This is more evident for larger tumors in which the burden of surgery is completely avoided. It can be applied in elderly, multimorbid patients on practically any concurrent medication. Besides optimal cosmesis, a distinctive advantage of immunocryosurgery in contrast to many other nonsurgical therapeutic modalities for skin cancer is that it is not carcinogenic. This side effect is a serious limitation of radiotherapy and potentially also connected to the use of topical antineoplastic agents. Finally, in immunocryosurgery, in contrast to ablative modalities, skin infections are of no concern at the treated sites. Particularly, no case of herpes simplex flare, an important side effect of many other modalities, has been observed.
The main drawback of this modality is the discomfort during treatment and the temporary cosmetic, sometimes also functional embarrassment caused by the inflammation on and around the treated lesion. Patients are encouraged to adhere to treatment by emphasizing the anticipated excellent cosmetic and functional outcome, which are guaranteed by this tissue-sparing modality.
Two special issues that are often encountered during immunocryosurgery and their management are shortly discussed in the following section as a guide to improve the applicability of the treatment in certain cases.
20.2.1 The “Right” Degree of Inflammation
A rather hefty inflammatory reaction of the treated area is generally a hallmark of a successful immunocryosurgery treatment. However, the degree of individual inflammatory reaction to the procedure is unpredictable. Thus, our target is to achieve a sustained inflammatory response that would not be as intense as to deter the patient from therapy. In almost all cases, even in those where the initial 14 days imiquimod course did not provoke a significant degree of local inflammation, this is induced after the cryosurgery session. In the unlikely case of absence of inflammation after cryosurgery, we add a topical retinoid in the treatment schedule (tazarotene or tretinoin once daily in the morning). However, more than absence of inflammation, usually our major concern mostly relates to the occasional immense inflammatory response, especially after the cryosurgery session. In addition, elderly patients are the main target group of this treatment and the treated neoplasm usually lies in photodamaged skin. The free application of imiquimod onto this field will result in areas of extended inflammation. In order to avoid this flair and optimize treatment, detailed instructions of how to control the applied imiquimod quantity per application is mandatory prior and during treatment.
20.2.2 Management of Side Effects
Adherence to instructions is pivotal for the success of immunocryosurgery, as, for example, in the treatment of basal cell carcinoma (BCC), we have observed an increased risk of treatment failure associated with skipping of imiquimod applications for various reasons (misunderstanding, lack of adherence to instructions, etc.), particularly in the last couple of days prior to the cryosurgery sessions. Thus, the key point for the success of the 5-week immunocryosurgery course is the establishment of a caring relationship towards the patient that would strengthen his trust in the physician and support adherence to the treatment. This includes the meticulous discussion of the treatment procedure prior to onset– also with the help of typical case photographs – and the anticipated side effects which constitute part of the treatment’s mode of action. Availability of the therapeutic team for extra consultations during the treatment period is essential. All through the treatment period, the patient should be reassured about the temporary nature of the discomfort caused and should be encouraged with the prospect of a favorable outcome with excellent cosmetic results.
In parallel to inflammatory reactions at the site of the treated lesion, usually low-grade systemic symptoms also emerge, which are more intense the week after the cryosurgery and gradually subside during ongoing treatment: low-grade fever in some patients, anorexia, or the feeling of tiredness in most of them, particularly those with larger lesions. As a rule, no antiseptic measures or antiviral medications for infection prophylaxis are required.
20.3 Indications of Immunocryosurgery
Immunocryosurgery is a relatively recent addition to the therapeutic modalities used to treat skin cancer [9], and the spectrum of indications is presently assessed. Immunocryosurgery has been mainly applied to treat skin neoplasms of keratinocytic origin with most experience concentrating in the treatment of BCC. Immunocryosurgery has been used both with primary curative as well as palliative therapeutic intension. Currently, the perspectives of the integration of this modality into treatment protocols for partially responding skin cancer are evaluated (e.g., combination with intralesional bevacizumab [10]). In the following sections, a short review of actual and potential indications of immunocryosurgery is presented (Table 20.1). Special aspects of the use of immunocryosurgery to treat skin lesions at certain anatomical localizations will be separately discussed later in this chapter.
Table 20.1
Indications of immunocryosurgery
1. Skin neoplasms of epithelial origin |
(a) Keratinocyte precancer and in situ SCC |
(i) Actinic keratoses |
(ii) Solar cheilosis (actinic cheilitis) |
(iii) Bowen’s disease of the skin |
(iv) Paget’s disease |
(v) Keratoacanthoma |
(b) Basal cell carcinoma |
2. Non-epithelial skin neoplasms |
(a) Lentigo maligna and MM |
(b) Kaposi sarcoma |
(c) Merkel cell carcinoma |
3. Benign skin growths and conditions |
(a) Genital warts |
(b) Pyogenic granuloma |
4. Potential applications |
(a) Skin metastases |
(b) Skin infections |
(c) Skin lymphoma |
(d) Hypertrophic scars and kelloids |
20.3.1 Skin Neoplasms of Epithelial Origin
Histopathological diagnosis, tumor size, and localization are the main neoplasm characteristics that together with the general health status and comorbidities/medications of the patient, frame the optimum treatment plan of an individual tumor in a certain patient. Especially the value of the precise histopathological diagnosis emerges as a core parameter for the newer modalities, including immunocryosurgery, in the expanding area of nonsurgical therapeutic interventions for malignant skin diseases.
20.3.1.1 Keratinocytic Precancer and In Situ SCC
Treatment outcome of these neoplasms with immunocryosurgery strongly depends on the stage of tumor progression. Overall high cure rates have been achieved with in situ neoplasms; however, the effectiveness against invasive squamous cell carcinomas (SCC) is highly unpredictable. This uncertainty underscores the need for accurate diagnosis.
Actinic Keratoses (AK)
Actinic keratoses can appear as single lesions or involve extensive skin areas (field cancerization) and are amenable to treatment with both cryosurgery and imiquimod [11]. Many authors regard cryosurgery as a first line modality for the treatment of most AK. Immunocryosurgery is highly effective in AK. Due to its vast efficiency and the involvement of large skin areas, we adapted the standard treatment protocol in order to minimize side effects and improve feasibility without reducing efficacy. Imiquimod is applied every other night for 2 weeks, with the patient applying it also the day prior to the cryosurgery session (Fig. 20.1b). Subsequently, mild cryosurgery is applied (open spray, liquid N2, 2 freeze-thaw cycles of 10 s each effective freezing time), and imiquimod is continued for another week on alternate days on the treated area, starting at the day of cryosurgery, i.e., for additional four times (a total of 11 imiquimod applications). In practice, this is guaranteed by providing the patients with a detailed calendar plan of imiquimod application. The patient is followed up, and treatment is repeated on persisting lesions. As in the case of BCC (see discussion later in this chapter), in the absence of inflammation, a local retinoid can be added as an adjuvant, once daily in the morning for the duration of the treatment.
Solar Cheilosis (Actinic Cheilitis)
A standard immunocryosurgery protocol has been used to treat cases of solar cheilosis (Spyridonos et al. 2014). Data with sufficient follow-up periods ≥1 year are available in 8 patients and demonstrate both feasibility and efficacy of the method. However, lip treatment with immunocryosurgery imparts a significant burden on the patient’s quality of life for the duration of treatment as local inflammation can prevent the patient from the consumption of solid food for the remaining period after the cryosurgery session. Based on our current experience, this approach is suggested exclusively for highly motivated patients and only after explicit explanation of the transient, yet significant, burden of the side effects of therapy.
Bowen’s Disease of the Skin (BD)
Both cryosurgery and imiquimod are moderately effective modalities for Bowen’s disease [12]. However, immunocryosurgery achieves excellent treatment outcomes in this condition (Fig. 20.2a–f) [13]. BD can sometimes be quite extensive or involve difficult-to-treat localizations, like the fingers [14], and immunocryosurgery can offer sufficient field therapy with excellent outcomes in these cases. Relatively small BD lesions are treated with the standard 5-week immunocryosurgery protocol. When larger areas are involved, especially on the head, the diseased area can be treated in subsections of 4–5 cm2. Monomodal cryosurgery can be employed for small sites of residual disease or recurrences within the treated area (up to 0.5 cm in diameter); for more extensive lesions immunocryosurgery can be repeated. In the literature, there is some concern about the possibility of BD progression to invasive SCC during imiquimod treatment [15]; however, to date such cases have not been observed with immunocryosurgery.
Keratoacanthoma
Immunocryosurgery might offer an efficacious alternative in the treatment of keratoacanthoma. Treatment with add-ins is suggested. Intralesional injection of 5-fluorouracil (50 mg in 1 ml solution) on day 0 followed by subsequent treatment with immunocryosurgery has been quite efficacious in inducing disease involution (unpublished data).
20.3.1.2 Squamous Cell Carcinoma (SCC)
The results of the treatment of squamous cell carcinoma (SCC) with immunocryosurgery are generally disappointing despite protracted and intensive treatment schedules used as palliative therapy in certain cases (unpublished data). In some of these patients, the tumor could be restricted in size; however, early relapses or even relapses under continuing treatment were observed, and thus this modality cannot be recommended for the treatment of SCC. Similar experience with progression of SCC during monomodal imiquimod treatment has been repeatedly reported in the literature [16–19], an additional argument against the use of this modality for SCC. This contrasts initial optimism regarding the use of imiquimod to treat SCC [20–23] and theoretical predictions about targeted imiquimod and cryosurgery actions on SCC [24] and also obviates the central value of clinical trials for the establishment of therapeutic indications. Moreover, the divergence in the susceptibility of basal cell carcinoma (BCC) and SCC to this therapeutic approach underscores the vast differences in biological nature and clinical behavior of these two families of keratinocytic neoplasms, a difference to date largely concealed because of the predominance of the pathophysiologically “indifferent” surgical-ablative approaches for the treatment of these lesions.
20.3.1.3 Basal Cell Carcinoma (BCC)
Locally Confined BCC
To date, most experience with the use of immunocryosurgery is in the treatment of locally confined BCC (Fig. 20.3a–h) [3–5, 8]. With one standard immunocryosurgery cycle, initial tumor clearance can be achieved in up to 97.5 % of unselected BCC with macroscopic diameter ≤2 cm, i.e., for the vast majority (80–90 %) of all BCC at the time of reference for treatment [25, 26]. Treatment is performed as detailed earlier in this chapter, with 15–20 s effective freezing time, and follow-up visits are scheduled at 1, 3, and 6 months after the end of treatment (end of imiquimod application), every 6 months for the rest first 2 years, and yearly thereafter. For comparing effectiveness with other treatment modalities, this single immunocryosurgery cycle can be considered as the equivalent of a conventional surgical excision with at least comparable therapeutic efficiency. In the few cases of incomplete (partial) responses with the repetition of this treatment cycle, tumor clearance is essentially achieved in all cases (>99 %) of primary and relapsed BCC ≤2 cm (Fig. 20.4a–f) [4]. This high clearance rate is coupled by the equally high cure rates with relapse free >97 % of the treated tumors 3 years after treatment. This effectiveness is significantly higher than (a) that reported for either monomodal imiquimod (<65 %; [27]) or cryosurgery (based on common experience probably <50 % for the herein applied treatment parameters; [compare: [28, 29]) and also (b) anticipated for the simple additive action of the two modalities [2]. It is worth noting that the core reasons for the reference of a BCC for Mohs’ surgery, i.e., recurrent tumor with poorly defined margins and located in a so-called high risk area [25], are no limitations for the application of immunocryosurgery [4]. Moreover, relapse rate profile compares successfully with corresponding outcomes after conventional surgery, after which relapse rates of 5–10 % are expected during follow-up [30].
Related posts:
 Preoperative Care for Cryosurgery
Preoperative Care for Cryosurgery
 Theoretical Principles of Immunocryosurgery
Theoretical Principles of Immunocryosurgery
 Cryobiopsy, Cryoanesthesia, and Cryoanalgesia
Cryobiopsy, Cryoanesthesia, and Cryoanalgesia
 In Vivo Reflectance Confocal Microscopy Assessment of Wound Induction and Repair of a Skin Injury Produced by Liquid Nitrogen: An Atlas
In Vivo Reflectance Confocal Microscopy Assessment of Wound Induction and Repair of a Skin Injury Produced by Liquid Nitrogen: An Atlas
 Cryosurgery for Warts
Cryosurgery for Warts
 Cryosurgery for Vascular Lesions
Cryosurgery for Vascular Lesions
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


