Key Words
breast reconstruction, implant, immediate, two-stage, acellular dermal matrix
Disclosure : The authors have no financial interest to declare in relation to the drugs, devices, and products mentioned in this article.
Introduction
There continues to be a steady annual growth in breast reconstruction within the United States, with over 100 000 procedures performed in 2016 and a 39% increase in reconstructive breast procedures since the year 2000.
Immediate two-stage prosthetic breast reconstruction is well accepted in breast cancer reconstruction due to its impact on post-mastectomy body image and quality of life, as well as its safety and high patient satisfaction. Furthermore, in 2010, a national survey found half of all US-based plastic surgeons who perform implant-based breast reconstruction use acellular dermal matrix (ADM). As prosthetic breast reconstructions continue to increase, all plastic surgeons should be well versed in delivering a safe, consistent, and aesthetically pleasing result in this kind of reconstruction.
In the following chapter, the authors will focus on tissue expander–based immediate breast reconstruction with acellular dermal matrix as a first-stage implant-based breast reconstruction. Emphasis will be placed on surgical technique, as well as highlighting key concepts and pearls in tissue expander/ADM-based reconstruction.
Indications and Contraindications
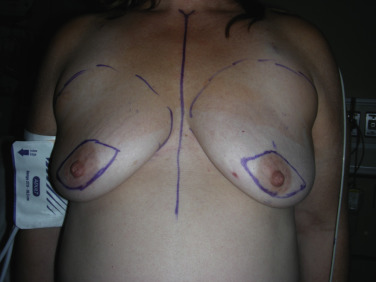
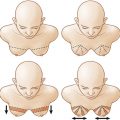
Treatment planning for post-mastectomy breast reconstruction depends on several issues. Key indications for immediate breast reconstruction include the patient’s oncologic disease burden as well as the need for adjuvant therapy. Immediate two-stage implant-based reconstruction is optimal in cases where adjuvant radiation therapy is not required. Ideal candidates include relatively thin patients and patients requiring bilateral reconstruction ( Fig. 10.1 ). However, the success and outcome of immediate implant-based reconstruction depends heavily on a reliable native soft tissue envelope. This can be achieved through a collaborative effort between the surgical oncologist and reconstructive surgeon. The two-stage approach also allows for precise recreation of the breast mound in terms of Infra-mammary fold (IMF) positioning, natural shape and final symmetry and is more flexible than one-stage implant-based reconstruction with fewer complications.

One absolute contraindication is ischemic or damaged mastectomy skin flaps. In this case a delayed reconstruction may be in the patient’s best interest. Other contraindications include poor quality of the pectoralis major muscle, obesity, and tobacco use.
Benefits of ADM
Acellular dermal matrices have become ubiquitous in breast reconstruction. The benefits of ADM include improved inframammary fold control, better support and control of the pocket, greater intraoperative expansion with fewer subsequent clinic visits, and decreased risk of capsular contracture. There is also evidence to suggest a clinical benefit for patients who undergo subsequent radiation therapy, but the literature remains inconclusive and will benefit from further studies.
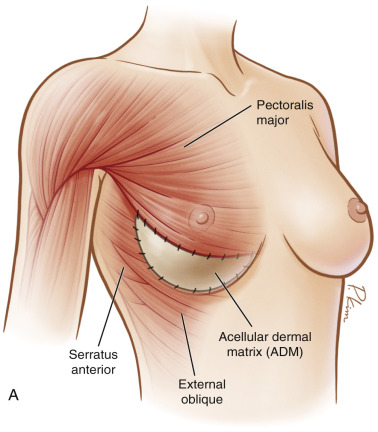
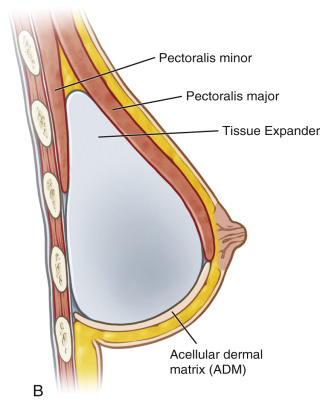
Additionally, by utilizing ADM as a tissue supplement over the inferior pole, further muscle dissection is spared, which leads to less postoperative pain, and a more anatomically precise pocket can be defined ( Fig. 10.2 ). The higherintra operative fill volume also addresses the retained skin in skin-sparing mastectomies. These benefits ultimately result in increased control by the surgeon over the reconstruction as well as final aesthetic outcome for the patient.
Preoperative Evaluation and Special Considerations
During the preoperative visit, the overall quality of breast skin in each patient should be evaluated carefully. In addition, the presence of breast ptosis should also be evaluated. One important discussion to highlight in the preoperative setting with the surgical oncologist is mastectomy flap thickness. It is imperative to adhere to good oncologic principles during the ablation. However, it must be emphasized that immediate prosthesis-based reconstruction relies on healthy and viable tissue flaps, which are to be respected in order to optimize the reconstructive outcome.
Skin-sparing or nipple-sparing mastectomy can usually be decided by the breast surgeon. The patient should be informed of the possibility of delayed reconstruction if the plastic surgeon deems the flaps are compromised. Additional considerations involve the impact of possible adjuvant chemotherapy and radiation therapy.
Surgical Techniques
Relevant Surgical Anatomy
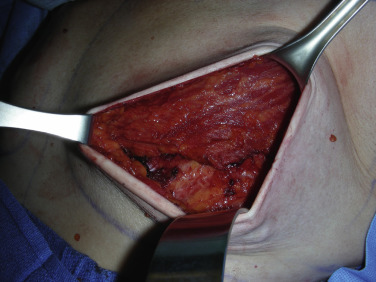
The mastectomy defect can vary with the approach to the soft tissue envelope. The most important consideration is the viability of the remaining skin flaps ( Fig. 10.3 ). As the skin relies on the dermal and subdermal plexus for its perfusion, any injury during the mastectomy from improper tissue handling or thermal cautery injury can lead to subsequent delayed wound healing or even reconstructive failure.

Once the breast parenchyma is removed, the pectoralis major muscle must be dissected free from its underlying attachments. This fan-shaped muscle has origins from the medial half of the clavicle, the sternum, the costal cartilage from the first to sixth ribs, and from the aponeurosis of the external oblique muscles. The fibers form two heads that course towards the insertion into the bicipital groove of the humerus. It is innervated by the lateral and medial pectoralis nerves and the blood supply is from the pectoral branch of the thoracoacromial artery. Deep to the pectoralis major muscle is its vascular pedicle, the pectoralis minor muscle and the chest wall and fibers from the external oblique . Care must be taken with dissection underneath the pectoralis major muscle to avoid injury to the above structures as well as major perforators from the internal mammary arteries. Finally, it is wise to avoid cautery dissection directly on top of the ribs, as this will lead to increased postoperative pain.
Preoperative Markings
Prior to surgery, the patient is marked in the standing position. The anatomic landmarks include the sternal notch, midline, clavicle, inframammary fold, and anterior axillary line. Specific attention must be paid to the inframammary fold as the inferior border of the mastectomy. The inframammary fold along with the medial, lateral and superior borders of the breast are marked. The skin-sparing skin pattern is also marked ( Fig. 10.4 ). Several options of expanders and acellular dermal matrix sizes are available but the final decision is made by the plastic surgeon intraoperatively after the mastectomy is completed. This ensures that each patient receives a reconstruction tailored to her individual needs.
Intraoperative Markings
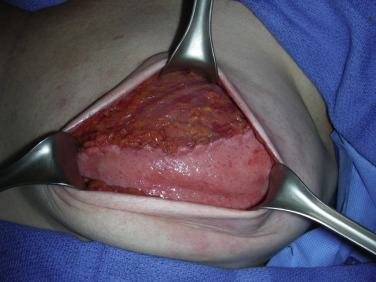
It is routine at our institution to begin reconstruction after the mastectomy is complete. The entire chest and axilla are re-prepped with betadine. It is always wise to inspect the mastectomy flaps for signs of thermal injury or full-thickness compromise ( Fig. 10.5 ). Often this can be mitigated with direct excision, but the decision to proceed must be made at this juncture, as compromised skin flaps may compromise the reconstruction entirely. Skin perfusion imaging may serve as an adjunct to clinical exam in determining skin flap viability. In addition, the quality of the pectoralis major muscle should also be inspected ( Fig. 10.6 ).


Next, the external breast border markings are transposed inside on top of the chest wall to help to restore the implant pocket. The two key areas are the inframammary fold and anterior axillary line, as this will define the dermal matrix sling and define the borders of the new breast. The transposed markings will also serve to guide suture placement for securing the ADM.
Details of the Procedure
Once the initial intraoperative markings are complete, the lateral edge of the pectoralis major muscle is identified. Using electrocautery, the dissection is started from the lateral extent. After the plane is identified between pectoralis major and the underlying chest wall, blunt finger dissection can be used to continue the dissection and elevate the muscle. It is common to encounter several perforators during the dissection, which should be cauterized.
Once the pectoralis major is sufficiently elevated ( Fig. 10.7 ), the sizing of the ADM can be approximated. The senior author uses rectangular ADM measuring 16 cm × 8 cm ultra-thick, and designs the matrix to lay parallel to the fibers of the pectoralis muscle. The excess corners of the dermal matrix are then cut to specification based on the preoperative markings along the IMF and lateral breast border ( Fig. 10.8 ).

Next, the ADM, with the dermal side facing up, is sutured in place using two 2-0 PDS sutures on a cutting needle. The steps of suture placement are key in ensuring precise pocket design, and are as follows. The first running suture begins in the inferior medial aspect; here the ADM is secured to Scarpa’s fascia to recreate the fold as well as to the pectoralis muscle. The suture is run in a simple interrupted fashion laterally as outlined by the transposed markings. The suture is then anchored in the superior lateral aspect. A bite is taken from the ADM to the deep pectoralis muscle fascia and to the substance of the serratus anterior fascia. This three-part stitch helps to close the implant pocket from the axilla. The second suture will be used in the final step to close the pocket once the tissue expander is in place. Continued running of the first suture is done to recreate the lateral border of the pocket, ending where the second suture is anchored.
The pectoralis and ADM pocket is then thoroughly irrigated with triple-antibiotic solution. Next, an appropriately sized expander is prepared by removing the air, soaking in triple antibiotic solution, then placing it within the pocket with a no-touch technique ( Fig. 10.9 ).
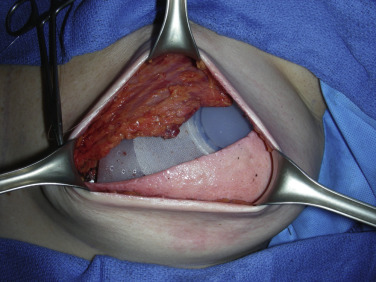
A medium high textured tissue expander is routinely selected in the senior author’s practice for the first-stage implant-based breast reconstruction. The expander is filled usually to approximately 120 cc with methylene blue injectable saline solution. The second running 2-0 PDS suture is then run down the ADM–pectoralis interface to close the pocket. At this point, additional expander fill is performed to obtain a snug fit within the pectoralis–ADM pocket without compromising muscle perfusion or overlying skin perfusion ( Fig. 10.10 ). In general, the expander can be filled to 50%–80% of its volume as long as mastectomy skin flap perfusion is not compromised ( Fig. 10.11 ).
Related posts:
 Immediate Implant Breast Reconstruction With Total Muscle Coverage – Two-Stage
Immediate Implant Breast Reconstruction With Total Muscle Coverage – Two-Stage
 Free Transverse Upper Gracilis Flap Breast Reconstruction
Free Transverse Upper Gracilis Flap Breast Reconstruction
 Fat Grafting as an Adjunct Procedure in Breast Reconstruction
Fat Grafting as an Adjunct Procedure in Breast Reconstruction
 Partial Breast Reconstruction With Local Tissue Rearrangements
Partial Breast Reconstruction With Local Tissue Rearrangements
 Fat Grafting for Total Breast Reconstruction
Fat Grafting for Total Breast Reconstruction
 Partial Breast Reconstruction With Flaps
Partial Breast Reconstruction With Flaps
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


