Key Words
Prepectoral breast reconstruction, subcutaneous breast reconstruction, surgical technique, complications, secondary procedures
Introduction
Prepectoral implant–based breast reconstruction is a recent addition to the breast reconstructive armamentarium that is rapidly being adopted given its simplicity and reported potential benefits. The technique involves placing the implant subcutaneously over the pectoralis major muscle, as opposed to under the muscle (subpectoral), which is the current established practice. By placing the implant over the pectoralis major muscle, the prepectoral approach preserves the anatomic integrity of the muscle as it is not dissected or elevated as in the subpectoral approach. With preservation of the muscle, the prepectoral approach eliminates animation deformity, pain, and muscle spasm that are often reported with elevating the muscle in the subpectoral approach. In addition, the prepectoral approach results in a natural-looking breast that anatomically resembles a native breast.
The prepectoral concept, however, is not a novel concept. Subcutaneous implant placement was attempted more than half a century ago when silicone implants were first introduced to the market. The technique, however, was soon abandoned when it became apparent that soft tissue coverage provided by the mastectomy flap alone was insufficient to support and maintain the implant above the muscle. Complications of bottoming out; implant migration; implant visibility, palpability, rippling, and wrinkling; and skin breakdown were, thus, common with this technique.
The renewed interest in the prepectoral or subcutaneous approach began after a number of technique and device advancements were introduced over the years in breast reconstructive surgery. Mastectomies became less aggressive, deviating from radical mastectomies to skin- and nipple-sparing mastectomies that preserved mastectomy flap perfusion and viability, which are critical for the prepectoral approach. Tissue perfusion devices became available that could assess perfusion in real time, providing an objective means of evaluating flap viability. The use of acellular dermal matrices (ADMs) for lower pole soft tissue coverage in the dual-plane approach eventually led to the idea that the matrix could be used to provide total implant coverage, obviating the need to elevate the pectoralis major muscle. Improvements in implant designs, such as the highly cohesive gel implants, which are associated with less rippling and wrinkling, meant that these complications which are concerns with prepectoral implant placement could be mitigated. Lastly, advances in autologous fat grafting techniques have permitted the use of autologous fat to provide additional soft tissue coverage that is often needed in the prepectoral approach to mask implant visibility and rippling. All of these advancements taken together are credited with making the prepectoral approach a reality.
The authors and others have shown that the prepectoral approach can be an effective reconstructive option, but careful patient selection and meticulous technique are critical for successful outcomes. This chapter reviews the indications/contraindications and technique principles related to the prepectoral approach.
Indications and Contraindications
In general, ideal candidates for immediate prepectoral breast reconstruction are those who have a normal body mass index (BMI), small to medium breasts, minimal co-morbidity, and well-perfused mastectomy flaps. Many patients do not have this “ideal” candidate profile as they may be thin or obese or have mammary hypertrophy. This does not mean that prepectoral reconstruction is contraindicated in these patients but rather that it may be challenging to perform.
The availability of well-perfused, viable, mastectomy skin flaps is the single most absolute requirement for immediate prepectoral reconstruction. Given the proximity of the implant to the skin flaps, compromised skin flaps can result in skin necrosis which, in turn, may lead to infection, implant extrusion, and reconstructive failure. For this reason, any patient characteristic or factor that compromises flap perfusion or quality is considered a contraindication to immediate prepectoral approach. Thus, patient co-morbidities such as a BMI greater than 40 kg/m 2 (morbid obesity), uncontrolled diabetes (HbA1c >7.5%) and active smoking are all contraindications to the immediate prepectoral approach. In addition, immunocompromised patients are also not suitable candidates because these patients are, in general, at increased risk of complications, particularly infectious complications. In patients with uncontrolled diabetes, prepectoral reconstruction can, however, be performed as a delayed procedure after controlling blood sugar with appropriate treatment. Likewise, obese patients (BMI >40 kg/m 2 ) without prior radiation therapy can be considered for delayed prepectoral reconstruction.
Immediate prepectoral reconstruction is generally not recommended in patients who have undergone prior breast irradiation, particularly if the lumpectomy scar is in the lower pole. Radiation damages the skin envelope and causes dermal thickening, thus increasing the risk of skin breakdown during the tissue expansion phase. Reconstructive options for these patients have traditionally relied on autologous approaches. However, an immediate, latissimus-based, prepectoral approach can be considered in these patients. The latissimus-based approach is typically performed in two stages (expander/implant), with or without soft tissue introduction with the flap depending on the need for supplemental soft tissue. The expander stage is critical in this approach to allow for skin and subcutaneous tissue expansion.
Post-mastectomy radiation therapy (PMRT), on the other hand, is not a contraindication to immediate prepectoral reconstruction. PMRT can be delivered to the expander or the implant as in the subpectoral approach. PMRT, in general, increases the risk of short- and long-term complications, including incisional dehiscence, infection, delayed healing, seroma, hematoma, capsular contracture, implant malposition/asymmetry, and reconstructive failure. Being cognizant of potential complications of PMRT is important as proactive management can improve patients’ chances of a good outcome.
Lack of fat depots is another contraindication for immediate prepectoral reconstruction. This is of particular concern in thin patients. Thin patients have thin skin flaps that may not be adequate to mask implant visibility and rippling and require autologous fat grafting to improve aesthetic outcomes. However, alternative soft tissue fillers are an option in those without fat depots, in which case immediate prepectoral reconstruction can be considered. Further, highly cohesive gel implants are associated with less rippling and their use in thin patients may help reduce implant-related complications.
In addition to the reconstructive indications/contraindications, a number of oncologic factors also need to be taken into consideration when contemplating immediate prepectoral reconstruction. Patients with large tumors (>5 cm), posterior tumors lying near the pectoralis major muscle, chest wall involvement, axillary involvement, late-stage breast cancer, and a high risk of recurrence are not candidates for prepectoral placement. The oncologic safety of prepectoral placement in these cases is not known and it would be prudent to adhere to a conservative, cautious approach to breast reconstruction in these patients. In patients with axillary involvement and late-stage breast cancer (stage IV), aggressive adjuvant therapies may be required which preclude the immediate reconstructive option.
It should be noted that the immediate reconstructive contraindications discussed above do not apply to delayed prepectoral reconstruction. In particular, flap viability and perfusion is not a requirement for delayed reconstruction. When considering patients for delayed prepectoral reconstruction, the overall health of the patient is taken into consideration.
Indications and Contraindications
In general, ideal candidates for immediate prepectoral breast reconstruction are those who have a normal body mass index (BMI), small to medium breasts, minimal co-morbidity, and well-perfused mastectomy flaps. Many patients do not have this “ideal” candidate profile as they may be thin or obese or have mammary hypertrophy. This does not mean that prepectoral reconstruction is contraindicated in these patients but rather that it may be challenging to perform.
The availability of well-perfused, viable, mastectomy skin flaps is the single most absolute requirement for immediate prepectoral reconstruction. Given the proximity of the implant to the skin flaps, compromised skin flaps can result in skin necrosis which, in turn, may lead to infection, implant extrusion, and reconstructive failure. For this reason, any patient characteristic or factor that compromises flap perfusion or quality is considered a contraindication to immediate prepectoral approach. Thus, patient co-morbidities such as a BMI greater than 40 kg/m 2 (morbid obesity), uncontrolled diabetes (HbA1c >7.5%) and active smoking are all contraindications to the immediate prepectoral approach. In addition, immunocompromised patients are also not suitable candidates because these patients are, in general, at increased risk of complications, particularly infectious complications. In patients with uncontrolled diabetes, prepectoral reconstruction can, however, be performed as a delayed procedure after controlling blood sugar with appropriate treatment. Likewise, obese patients (BMI >40 kg/m 2 ) without prior radiation therapy can be considered for delayed prepectoral reconstruction.
Immediate prepectoral reconstruction is generally not recommended in patients who have undergone prior breast irradiation, particularly if the lumpectomy scar is in the lower pole. Radiation damages the skin envelope and causes dermal thickening, thus increasing the risk of skin breakdown during the tissue expansion phase. Reconstructive options for these patients have traditionally relied on autologous approaches. However, an immediate, latissimus-based, prepectoral approach can be considered in these patients. The latissimus-based approach is typically performed in two stages (expander/implant), with or without soft tissue introduction with the flap depending on the need for supplemental soft tissue. The expander stage is critical in this approach to allow for skin and subcutaneous tissue expansion.
Post-mastectomy radiation therapy (PMRT), on the other hand, is not a contraindication to immediate prepectoral reconstruction. PMRT can be delivered to the expander or the implant as in the subpectoral approach. PMRT, in general, increases the risk of short- and long-term complications, including incisional dehiscence, infection, delayed healing, seroma, hematoma, capsular contracture, implant malposition/asymmetry, and reconstructive failure. Being cognizant of potential complications of PMRT is important as proactive management can improve patients’ chances of a good outcome.
Lack of fat depots is another contraindication for immediate prepectoral reconstruction. This is of particular concern in thin patients. Thin patients have thin skin flaps that may not be adequate to mask implant visibility and rippling and require autologous fat grafting to improve aesthetic outcomes. However, alternative soft tissue fillers are an option in those without fat depots, in which case immediate prepectoral reconstruction can be considered. Further, highly cohesive gel implants are associated with less rippling and their use in thin patients may help reduce implant-related complications.
In addition to the reconstructive indications/contraindications, a number of oncologic factors also need to be taken into consideration when contemplating immediate prepectoral reconstruction. Patients with large tumors (>5 cm), posterior tumors lying near the pectoralis major muscle, chest wall involvement, axillary involvement, late-stage breast cancer, and a high risk of recurrence are not candidates for prepectoral placement. The oncologic safety of prepectoral placement in these cases is not known and it would be prudent to adhere to a conservative, cautious approach to breast reconstruction in these patients. In patients with axillary involvement and late-stage breast cancer (stage IV), aggressive adjuvant therapies may be required which preclude the immediate reconstructive option.
It should be noted that the immediate reconstructive contraindications discussed above do not apply to delayed prepectoral reconstruction. In particular, flap viability and perfusion is not a requirement for delayed reconstruction. When considering patients for delayed prepectoral reconstruction, the overall health of the patient is taken into consideration.
Preoperative Evaluation
Patient selection for immediate prepectoral reconstruction is governed by preoperative patient characteristics, co-morbidities, neoadjuvant therapies, cancer stage, and tumor location as well as intraoperative mastectomy flap perfusion and viability. The patient’s BMI, HbA1c status, and smoking history are assessed and information regarding cancer stage, tumor location, and neoadjuvant therapies are obtained from patient records. In the absence of contraindications, as outlined above, patient eligibility is ascertained provisionally. Following mastectomy, assessment of flap viability is performed intraoperatively. Prepectoral reconstruction is only offered if patients have well-perfused mastectomy flaps. As alluded to above, well-perfused mastectomy flaps are an absolute requirement for the immediate prepectoral approach.
Assessment of flap vascularity and viability is ideally performed objectively with the use of a tissue perfusion assessment device. Several of these devices are currently available, most of which use indocyanine green angiography to visualize arterial and venous flow in real time. These devices not only allow the assessment of tissue viability but also help identify areas of compromised perfusion, allowing their immediate excision to minimize tissue damage.
When a perfusion assessment device is not available or easily accessible, flap viability is ascertained by clinical assessment. Clinically, a well-perfused flap is recognized by bleeding incision margins and the presence of a layer of subcutaneous tissue under the flap. The latter is indicative of a preserved subdermal vascular plexus, which suggests the overlying flap is likely to be perfused and viable. A visible dermis under the skin flap suggests that the flap is too tenuous and not likely to be well perfused and viable. Skin flap thickness should not be used to assess for flap viability because skin thickness does not necessarily correlate to tissue viability.
In order to ensure the integrity of skin flap perfusion following mastectomy, a close collaboration with the general/oncologic surgeon is undertaken preoperatively. The general surgeon is briefed about the subsequent reconstructive approach so that aggressive mastectomies that compromise the vascularity of the mastectomy flaps are avoided as much as possible.
Surgical Techniques
Overall, the prepectoral technique is simpler than the subpectoral technique as chest wall muscles are not elevated. Nonetheless, attention to technique principles pertaining to pocket to implant dimensions, acellular dermal matrix in setting, prosthesis dynamics, and aseptic conditions is critical for successful outcomes.
Following mastectomy and ascertaining flap perfusion and viability, the patient’s internal breast dimensions are assessed in order to determine the size and dimension of the final implant. The final implant should fit snugly into the mastectomy pocket or prepectoral space. An implant that is smaller than the pocket creates dead space which increases the risk of seroma formation. Additionally, the lax overlying skin flap increases the risk of implant rippling and wrinkling. An implant that is larger than the pocket, on the other hand, places undue stress on the overlying flap and increases the risk of skin necrosis and its attendant consequences of infection, implant extrusion, and reconstructive failure. Reconstruction can be performed in one or two stages depending on patient preference, co-morbidities (BMI), and flap thickness. The advantage of the two-stage approach is that pocket adjustments can be made at the second stage, ensuring a snug fit of the implant that would otherwise have to be performed as a secondary procedure in the one-stage approach.
After establishing the implant dimensions, a footprint of the future breast is created by marking the position of the medial and lateral borders and inframammary fold on the outside and inside of the mastectomy pocket to help guide prosthesis placement. Attention is then focused on optimizing the pocket to accommodate the future implant. Subcutaneous tissue is repositioned to fill the spaces and collapse the pocket, as needed, to eliminate dead space. Dead space is more of a concern in obese patients and can be quite extensive following mastectomy. The removal of breast tissue in obese patients leads to the descent of large depots of lateral subcutaneous tissue to the posterior axillary line and the retraction of cephalad-subcutaneous tissue. The lateral subcutaneous tissue is displaced and secured to the anterior axillary line which collapses the pocket laterally. This decreases the risk of indentations that can form in these patients with thick subcutaneous tissue and decreases the risk of seroma formation laterally. The cephalad-subcutaneous tissue is displaced and secured caudally, which further collapses the pocket.
Acellular dermal matrix is integral to prepectoral reconstruction. The matrix is placed and secured over the entire anterior surface of the prosthesis. When used in this capacity, the matrix replaces the pectoralis major muscle, which is elevated to cover the prosthesis in the subpectoral approach. The matrix provides an additional layer of tissue support to the prosthesis and helps reduce the risk of bottoming out, prosthesis extrusion, inframammary fold malposition, rippling/wrinkling, and device visibility. It also mitigates the risk of capsular contracture and implant malposition in the long term. Typically, a single thick (2–3 mm) sheet of perforated acellular matrix measuring 16 cm × 20 cm is utilized for each breast. If using other sizes of matrix, two sheets may be required, which are sutured together with absorbable sutures to create one large sheet before insetting. In all cases, the acellular matrix is prepared according to the manufacturer’s specifications before use.
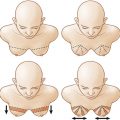
The technique of insetting of the acellular matrix varies depending on the incision location. In the case of an inframammary or lateral incision, the matrix is inset and secured to the pectoralis major muscle beginning superiorly and descending inferiorly on both sides toward the inframammary fold. Laterally, the matrix is secured to the serratus fascia while medially it is secured to the pectoralis major muscle. It is not secured inferiorly at this stage. The prosthesis is introduced into the pocket under the matrix through the inframammary fold incision and is secured directly onto the pectoralis major muscle via suture tabs. The matrix is draped over the inferior portion of the prosthesis and a 3–4 cm cuff is tucked under the prosthesis. The fold of the matrix is secured to the chest wall creating the inframammary fold. In the case of a transverse incision, the matrix is sutured inferiorly to the chest wall along the inframammary fold, leaving a 3–4 cm cuff toward the pectoralis major muscle. The prosthesis is introduced into the pocket and secured onto the pectoralis major muscle via suture tabs. The matrix is draped over the prosthesis and secured to the pectoralis major muscle medially and superiorly and to the serratus fascia laterally. The 3–4 cm cuff in both techniques serves to reinforce, stabilize, and define the inframammary fold and also support and stabilize the prosthesis and prevent bottoming out. In addition to these two techniques of acellular matrix placement, there are other techniques that utilize prefabricated prosthesis–matrix constructs. In these constructs, the prosthesis is completely covered anteriorly and to varying extent posteriorly with the matrix prior to its introduction into the mastectomy pocket. These “wrapped” constructs are currently not approved by the US Food and Drug Administration.
If using a tissue expander, it is partially inflated after insertion and before completion of securing the matrix. Typically, expanders are inflated to 50%–70% of maximum capacity with saline or air. Inflation with air is an off-label technique but is the author’s preferred technique. As air is lighter than saline, it helps alleviate the pressure on the inferior mastectomy flap and minimize suture pull-through. Under-filling also helps to alleviate the pressure on the overlying flap, reducing the risk of ischemia, which is more of a concern with thinner than thicker flaps. Thinner flaps, in general, are more sensitive to compression. Real-time flap perfusion angiography can be used to guide intraoperative expansion and ensure that perfusion is not compromised. Under-filling, however, should not create dead space or compromise the apposition of the acellular matrix to the overlying skin flap. Adequate contact between the matrix and the skin flap is critical for matrix revascularization, recellularization, and incorporation into host tissue. However, the matrix should not be pulled taut over the prosthesis but should have some laxity to accommodate for subsequent tissue expansion. Typically a tissue expander with a base width that is 0.5–2 cm smaller than the base width of the final implant is utilized so as to ensure a snug fit of the final implant. In one-stage reconstructions, an implant that conforms to the exact dimensions of the future footprint of the breast pocket is utilized and the acellular matrix is sutured taut over the implant without laxity.
In selecting the final implant for the prepectoral approach, implant cohesivity and/or fill capacity are important considerations. Form-stable, highly cohesive gel implants and high-fill implants are generally associated with less rippling and are thus the preferred implants in the prepectoral approach. Implant selection is a shared decision between the surgeon and the patient. As the shape and form of the reconstructed breast is dictated by the implant, the patient should be comfortable with the expected outcome. Surgeons should discuss the cohesivity of available implants and the trade-offs associated with using each implant type with patients.
Drains are essential in the prepectoral as in the subpectoral approach to reduce the risk of seroma. Seroma is of particular concern when using large pieces of acellular matrix. Typically two drains are placed between the matrix and the skin flap. Use of perforated matrices may further facilitate drainage and mitigate seroma risk.
In two-stage reconstructions, expanders are exchanged for permanent implants at about 3 months in patients who do not require adjuvant therapy. The expander is accessed preferably via an inframammary incision. After implant exchange, two drains are placed as in the first stage. At both stages, skin closure is performed in standard fashion in layers using absorbable sutures.
Strict sterile conditions should be maintained at all times during prepectoral reconstruction to reduce the risk of infectious complications. Following mastectomy, the prepectoral space is irrigated with a triple antibiotic cocktail (1 g cefazolin, 80 mg gentamicin, 50 000 IU bacitracin in 500 cc of normal saline) and again before prosthesis insertion. The prosthesis is also rinsed in the same antibiotic solution before insertion. Handling of the prosthesis is minimized and gloves are changed before handling the prosthesis. Antibiotics are administered pre-, intra-, and postoperatively to further mitigate the risk of infection per standard protocol.
Related posts:
 Immediate Implant Breast Reconstruction With Total Muscle Coverage – Two-Stage
Immediate Implant Breast Reconstruction With Total Muscle Coverage – Two-Stage
 Free Transverse Upper Gracilis Flap Breast Reconstruction
Free Transverse Upper Gracilis Flap Breast Reconstruction
 Fat Grafting as an Adjunct Procedure in Breast Reconstruction
Fat Grafting as an Adjunct Procedure in Breast Reconstruction
 Partial Breast Reconstruction With Local Tissue Rearrangements
Partial Breast Reconstruction With Local Tissue Rearrangements
 Fat Grafting for Total Breast Reconstruction
Fat Grafting for Total Breast Reconstruction
 Partial Breast Reconstruction With Flaps
Partial Breast Reconstruction With Flaps
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


