Key Points
- •
Indocyanine green (ICG) lymphography clearly visualizes superficial lymph flows in real time without ionized radiation exposure.
- •
Dynamic ICG lymphography, dual-phase fluorescent image observation, is important to maximize the efficacy of ICG lymphography for lymphatic mapping and appropriate severity staging.
- •
ICG lymphography findings change from “linear,” to “splash,” to “stardust,” and finally to “diffuse” pattern with the progression of lymphedema.
- •
ICG lymphography allows pathophysiologic severity staging for secondary lymphedema and classification of primary lymphedema.
Introduction
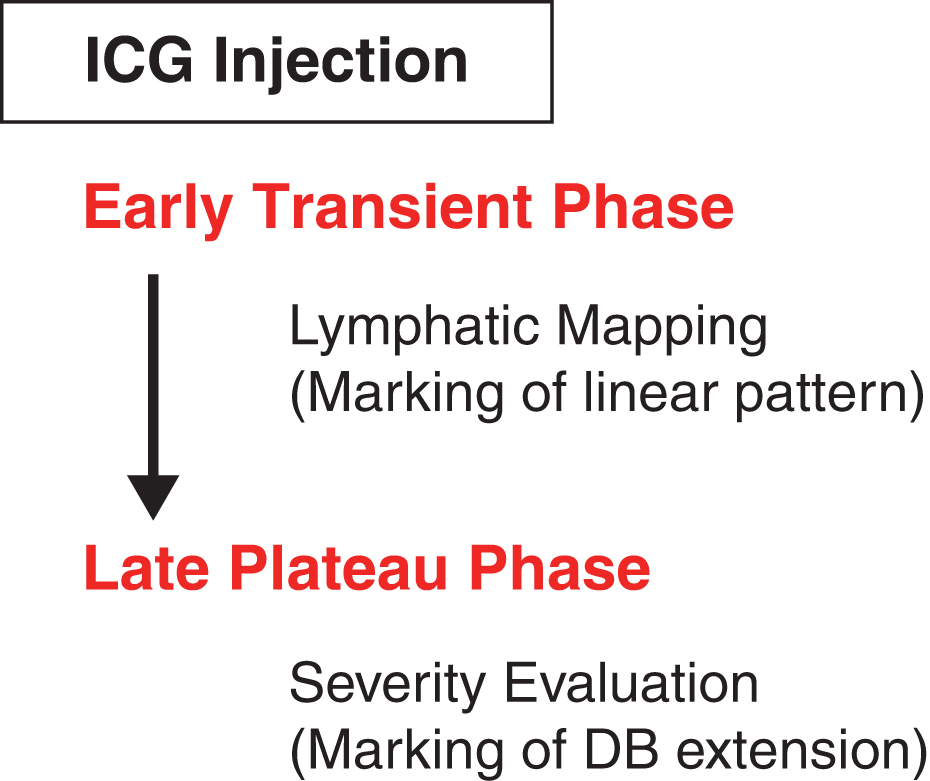
Although lymphoscintigraphy is considered a gold standard for lymph flow imaging, there are many drawbacks in lymphoscintigraphy necessitating another modality; obtained images are obscure and it has a risk of ionized radiation exposure. Near-infrared fluorescent lymphography using indocyanine green (ICG), or ICG lymphography, has been developed for lymphedema evaluation. ICG lymphography is becoming popular, since it allows much clearer visualization of superficial lymph circulation than other imaging modalities. As ICG lymphography allows real-time fluorescent imaging, pre/intraoperative navigation for lymphatic surgeries can be applied with the use of ICG lymphography into lymphaticovenular anastomosis (LVA), vascularized lymph node transfer (LNT), lymph-interpositional-flap transfer (LIFT), and liposuction in various parts of lymphedema, such as arm, leg, facial, and genital lymphedema. Dynamic ICG lymphography, dual-phase ICG lymphography, has been developed to allow pathophysiologic lymphedema evaluation and intraoperative mapping/navigation of lymphatics with only one ICG injection ( Fig. 7.1 ).
Characteristic ICG Lymphography Findings
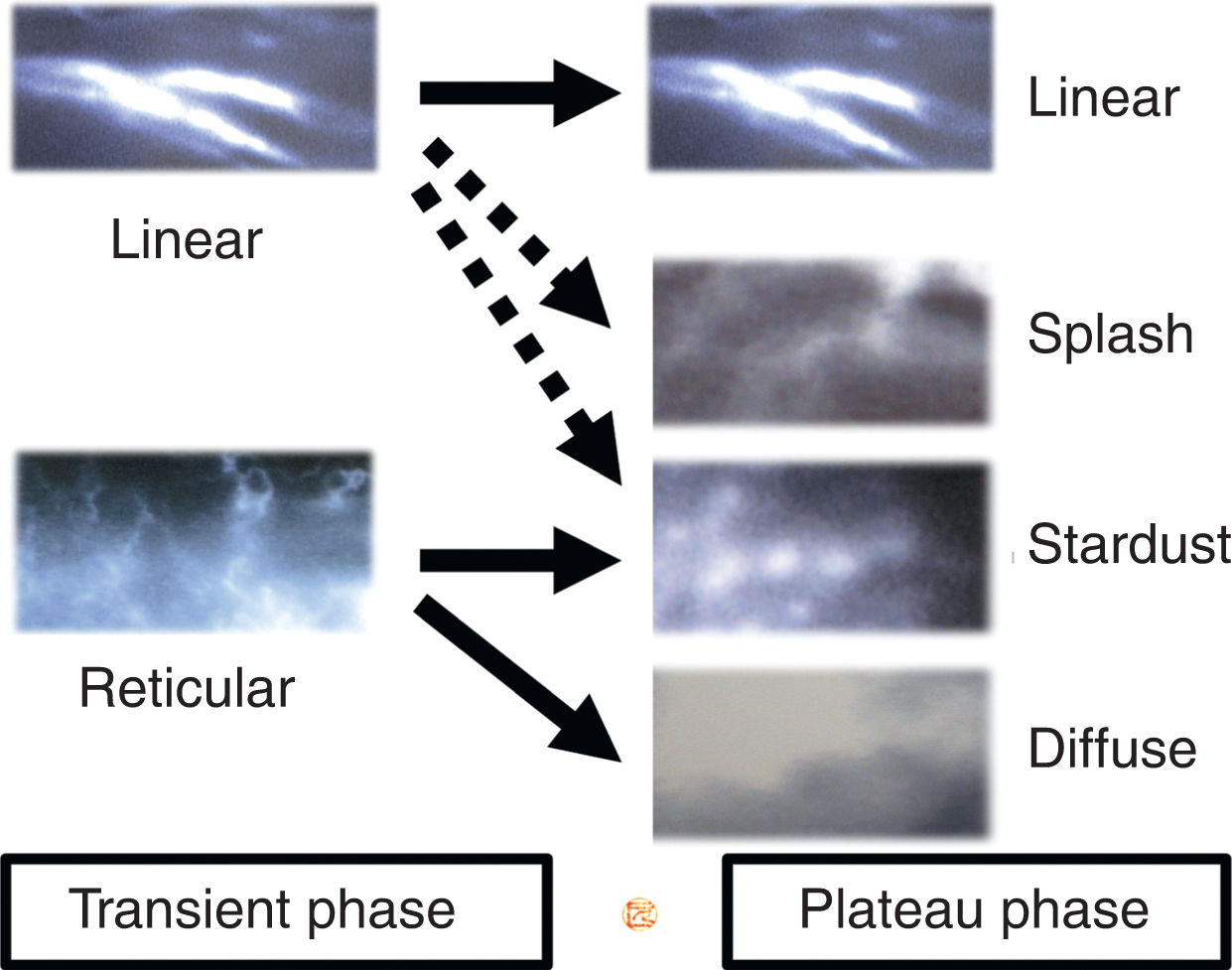
ICG lymphography findings are classified into two patterns: the normal “linear” pattern and the abnormal “dermal backflow (DB)” pattern. The DB pattern can be subdivided into “reticular,” “splash,” “stardust,” and “diffuse” patterns. The reticular pattern is an atypical DB pattern seen at an early transient phase, whereas splash, stardust, and diffuse patterns are DB patterns seen at a late plateau phase; the reticular pattern seen at a transient phase may change to a stardust or diffuse pattern at a plateau phase ( Fig. 7.2 ). The linear pattern, longitudinal lines along the axis of the extremity, represents lymph flows of the collecting lymphatic vessels, normograde lymph flows. Damage to lymph nodes or vessels, such as by lymph node dissection, radiation, trauma, or malformation, causes lymphatic hypertension, dilatation of the collecting lymphatic vessels, lymphatic valvular insufficiency, and retrograde lymph flows. Retrograde lymph flows of the superficial collecting or the precollecting lymphatic vessels are shown as a splash pattern of tortuous lines on ICG lymphography. These dilated superficial lymphatics play as collateral lymphatic pathways. When the collateral pathways fail to compensate for lymphatic overload, further retrograde lymph flows take place, leading to vertical retrograde flows toward the dermis. These vertical retrograde lymph flows are shown as spots on ICG lymphography: the stardust pattern. Finally, the collecting and precollecting lymphatic vessels can be obstructed because of lymphosclerosis, and horizontal lymph flows of the dilated lymphatic capillaries play a major role in lymph circulation. These dilated lymphatic capillaries are shown as a diffuse pattern, diffusely enhanced on ICG lymphography.
Dynamic ICG Lymphography
Dynamic ICG lymphography is performed with one ICG injection and two fluorescent image observations, in which 0.05–0.2 mL of 0.025–0.25% ICG is subdermally injected: each 0.2 mL at the second web space of the foot and posterior to the medial/lateral malleolus for lower extremity and genital lymphedema, each 0.1 mL at the second web space of the hand and ulnar/radial to the palmaris longus tendon (at the wrist level) for upper extremity lymphedema, and 0.05 mL each at the glabella and the philtrum for facial lymphedema. The concentration of ICG is changed according to the sensitivity of the ICG fluorescent image of a near-infrared camera system. Basically, a handheld camera system has higher sensitivity than a camera-integrated microscope system does; a higher concentration is recommended for preoperative or intraoperative visualization of lymph vessels using a camera-integrated microscope system.
At an early transient phase, immediately after ICG injection, fluorescent images are obtained to localize the collecting lymph vessels by marking a linear pattern with a pen. Since the reticular pattern is seen only at the transient phase and eventually changes to a stardust or diffuse pattern at the plateau phase, only linear pattern should be marked at the transient phase. As lymphatic vessels’ conditions are different according to DB patterns, differentiation of stardust and diffuse patterns is important; extension of the reticular pattern should not be marked at this phase, and extensions of stardust and diffuse patterns should be separately marked at the plateau phase.
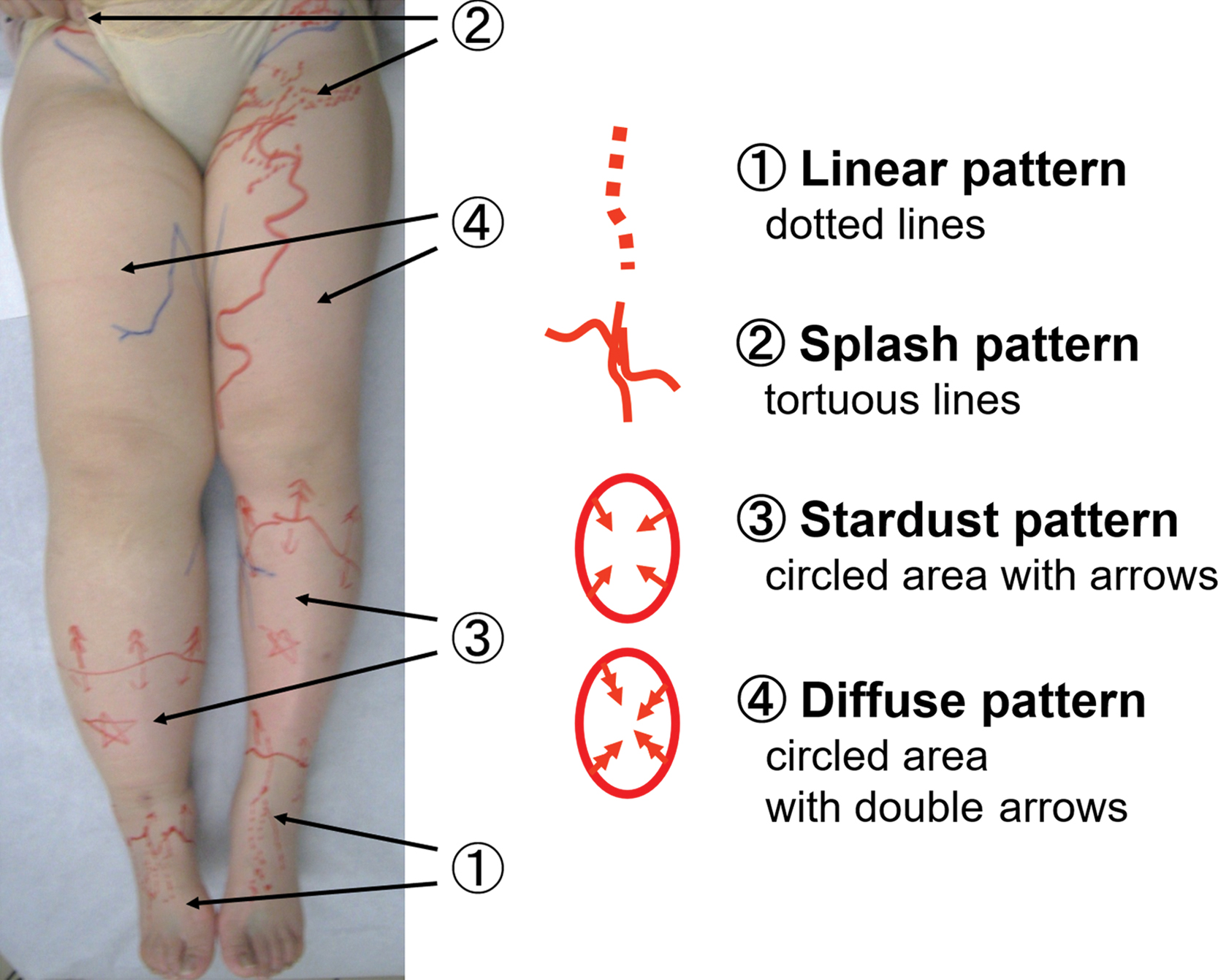
At a late plateau phase, 2–72 hours after ICG injection, ICG movement reaches a plateau; for severe lymphedema cases, a patient should move the affected limbs rigorously, because it usually takes longer time for ICG movement to reach a plateau. Differentiation and extension of each DB pattern are evaluated at this phase. DB patterns are marked so that differentiation (splash, stardust, or diffuse pattern) and extension of each DB pattern are easily understood at a glance ( Fig. 7.3 ). ICG lymphography severity staging should be based on findings at a plateau phase, not based on those at a transient phase, as described later.
ICG Lymphography Severity Staging for Secondary Lymphedema
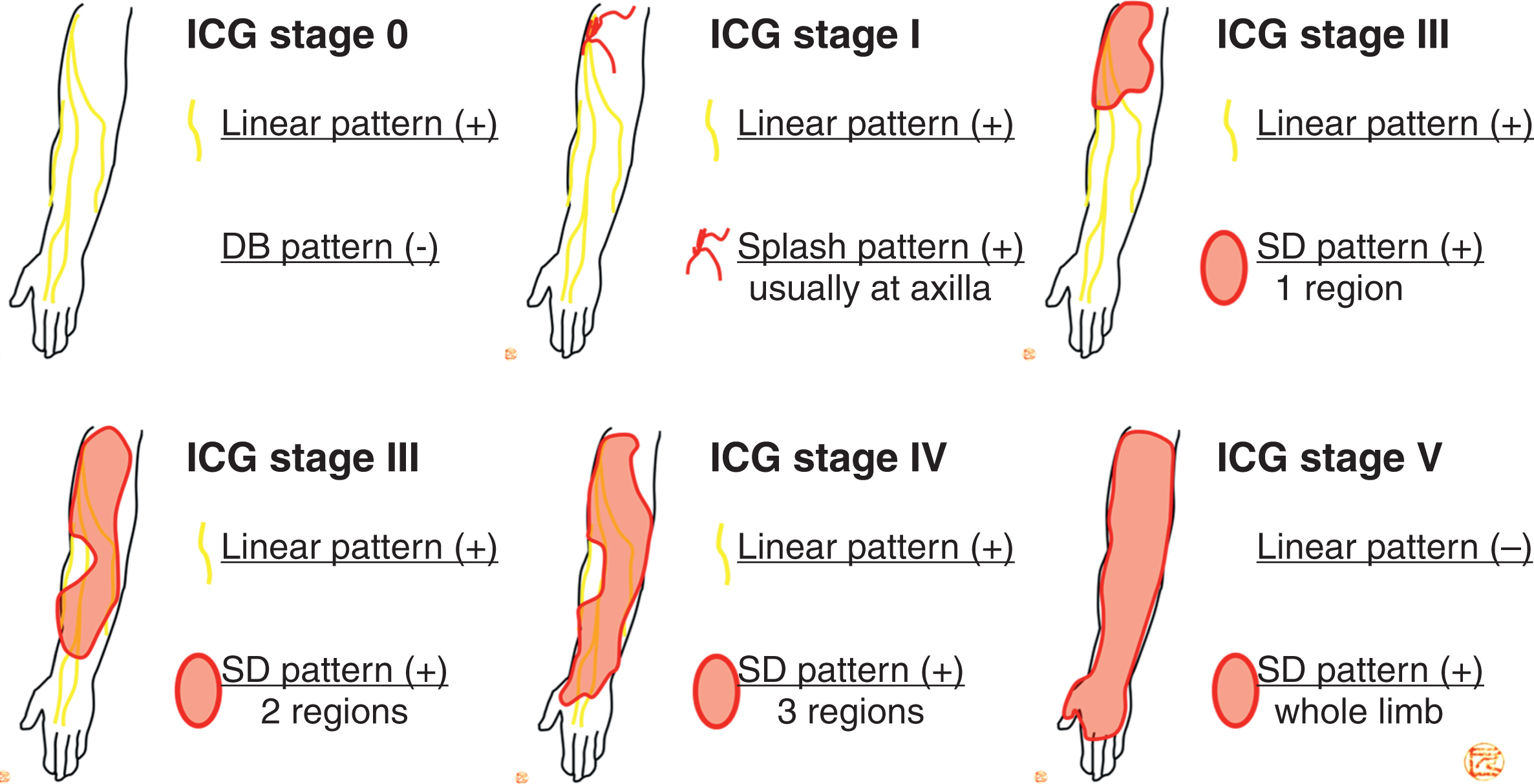
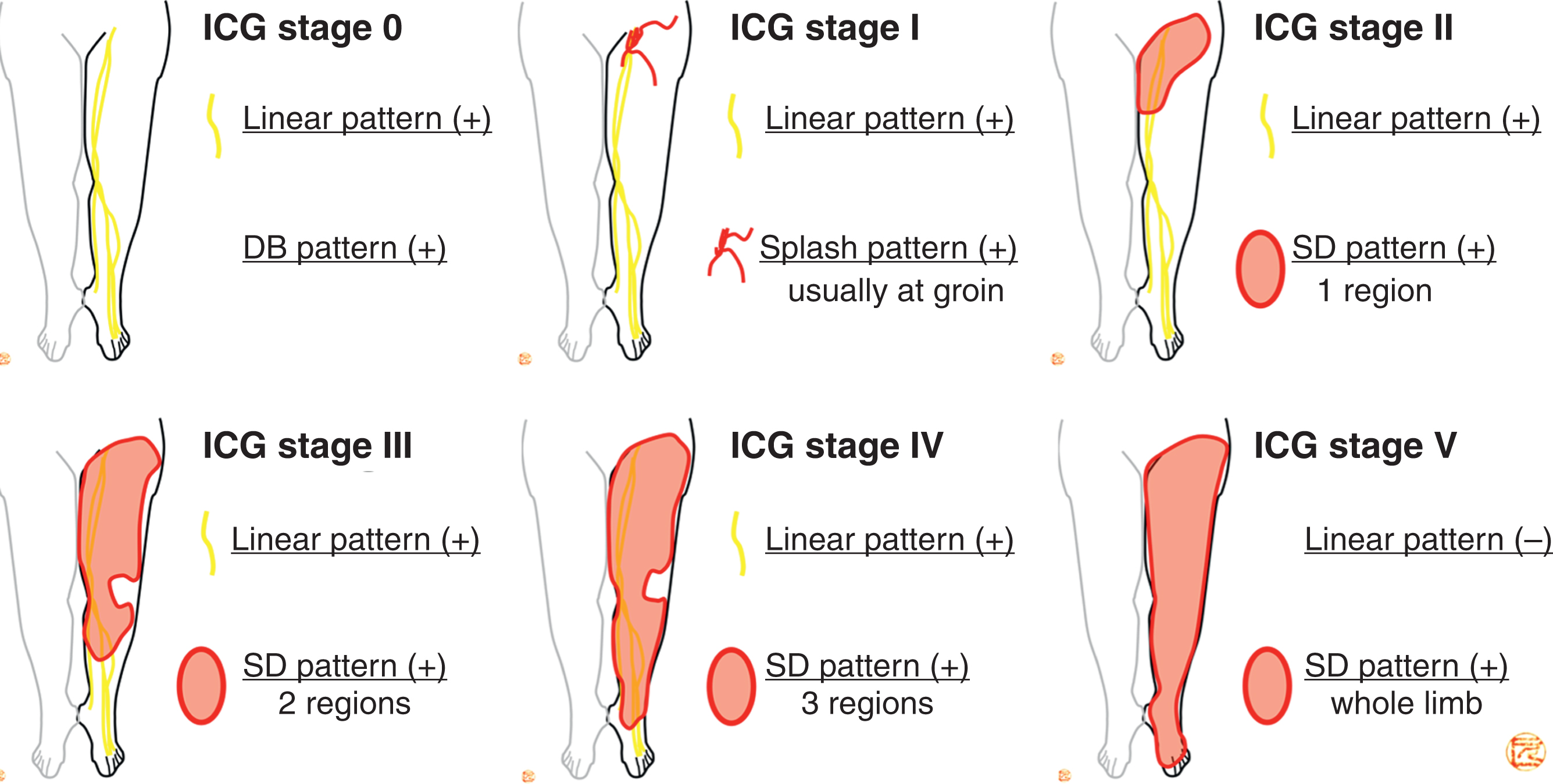
Pathophysiologic ICG lymphography stages, or modified DB stages for secondary lymphedema, are determined according to the visibility of a linear pattern and the extension of DB patterns. The ICG stage is applicable for secondary lymphedema of the upper extremity, the lower extremity, the face/head/neck, and the lower abdomen/genitalia. ICG staging consists of stage 0 through stage V ( Table 7.1 ).
| ICG Stage | ICG Lymphography Findings |
|---|---|
| Stage 0 | Linear pattern only (no DB pattern) |
| Stage I | Linear pattern+splash pattern * |
| Stage II | Linear pattern+SD pattern (one region) |
| Stage III | Linear pattern+SD pattern (two regions) |
| Stage IV | Linear pattern+SD pattern (three regions) |
| Stage V | SD pattern only (no linear pattern) |
* The splash pattern is usually seen in the most proximal region from the obstruction, site such as the groin, the axilla, and the neck.
First, each body part is divided into three regions: upper arm, forearm, and hand for upper extremity lymphedema; thigh, lower leg, and foot for lower extremity lymphedema; upper face (above the level of the palpebral fissure), lower face (the mandibular margin to the level of the palpebral fissure), and neck for facial lymphedema; and lower abdomen (umbilicus to the pubic tubercle), labia majora or scrotum, and labia minora or penis for genital lymphedema. For all ICG stages (upper/lower extremity, facial, and genital lymphedema), these classifications of regions are used to determine the severity stage.
In ICG stage 0, only the linear pattern is seen, and no DB pattern is detected—no lymphedema. In ICG stage I, the splash pattern is seen in addition to the linear pattern and is usually observed in the region most proximal to the obstruction site, such as the groin for lower extremity lymphedema secondary to pelvic lymph node dissection. ICG stage I represents subclinical lymphedema; around 30% of subclinical lymphedema cases spontaneously down-stage to stage 0 without any treatment, whereas the remaining 70% stay in stage I or progress to stage II. In ICG stage II–IV, the linear pattern and the stardust/diffuse (SD) pattern are observed. One region shows an SD pattern in ICG stage II, two regions in ICG stage III, and three regions in ICG stage IV. In ICG stage V, the SD pattern is seen in all regions, and the linear pattern is not detected; the difference between ICG stage IV and stage V is the visibility of the linear pattern. ICG stage II represents early lymphedema, while ICG stage III–V represents progressed lymphedema ( Figs. 7.4 and 7.5 ).
Since primary lymphedema has a wide variety of etiologies, not only lymph flow obstruction, ICG severity stage is used mainly for secondary lymphedema. However, for primary lymphedema with DB patterns (proximal and distal DB types), the ICG stage can be applied for severity staging.
ICG Lymphography Classification for Primary Lymphedema
ICG lymphography alone is not recommended for primary lymphedema evaluation. ICG lymphography visualizes only superficial lymph flows, and deep lymph flows in the thoracic and the abdominal cavity should be evaluated in primary lymphedema. Single photon emission computed tomography/computed tomography (SPECT/CT) lymphoscintigraphy and/or magnetic resonance lymphography are needed for thorough evaluation of lymph circulation. Although not an optimal imaging study, ICG lymphography is still of clinical usefulness with practical differentiation of primary lymphedema. ICG classification of primary lymphedema includes four types: proximal DB (PDB) type, distal DB (DDB) type, less enhancement (LE) type, and no enhancement (NE) type. Each type has different lymphographic and clinical characteristics ( Fig. 7.6 , Table 7.2 ).
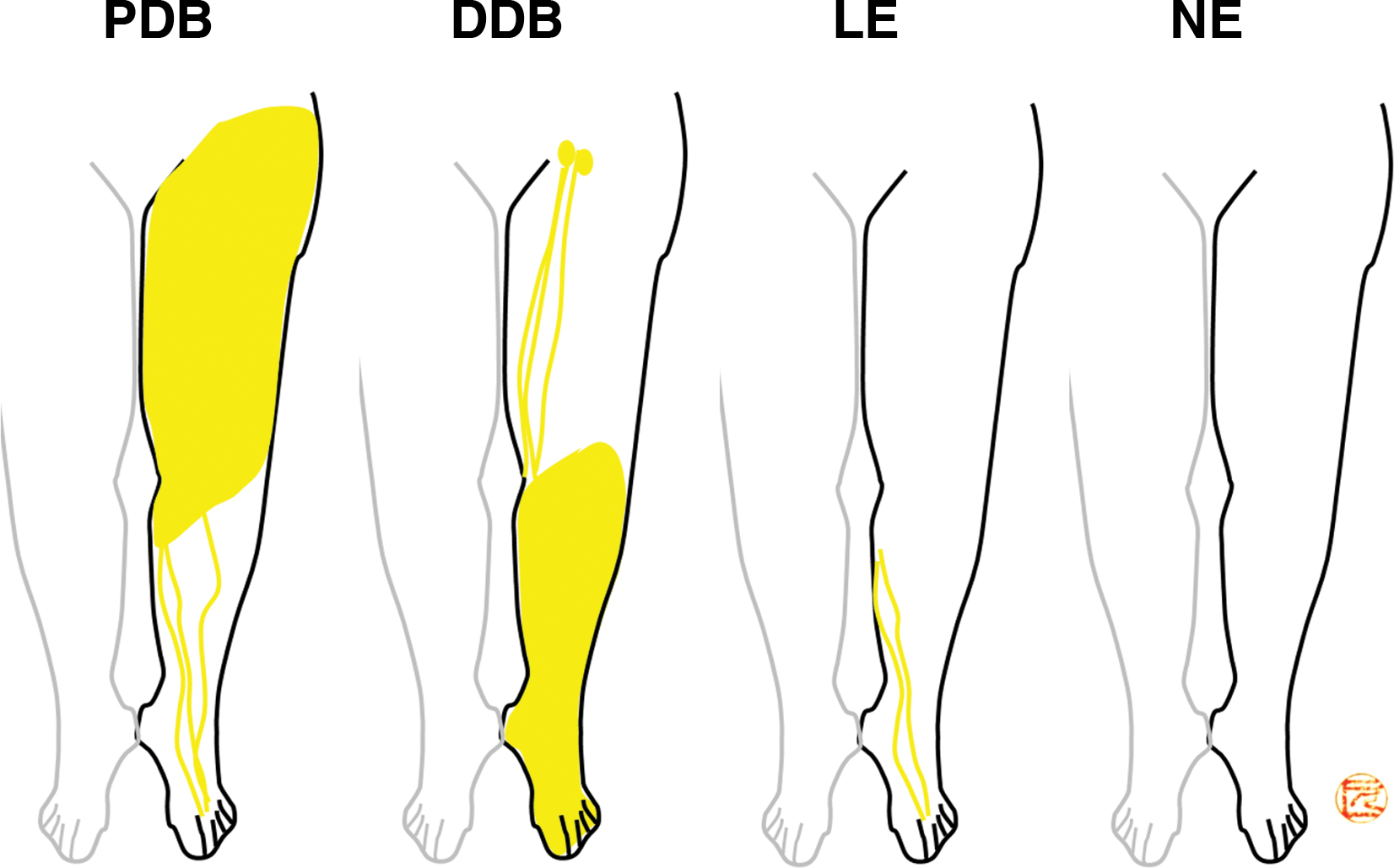
| ICG Type | ICG Lymphography Findings |
|---|---|
| PDB type | DB pattern extends from the proximal to the distal region. |
| Linear pattern may be seen in the distal region. | |
| DDB type | DB pattern is seen only in the distal region. |
| Linear pattern is seen in the proximal region. | |
| LE type | Linear pattern is seen only in the distal region. |
| No DB is detected (no enhancement in the proximal region). | |
| NE type | No enhancement is detected other than the ICG injected site. |
Related posts:
 Lymphoscintigraphy Interpretation, Staging, and Lymphedema Grading
Lymphoscintigraphy Interpretation, Staging, and Lymphedema Grading
 Anatomy and Structural Physiology of the Lymphatic System
Anatomy and Structural Physiology of the Lymphatic System
 Microsurgical Procedures: Vascularized Lymph Node Transfer from the Submental Region
Microsurgical Procedures: Vascularized Lymph Node Transfer from the Submental Region
 Private: The Campisi Approach for Lymphatic Surgery
Private: The Campisi Approach for Lymphatic Surgery
 Private: Tracking Outcomes Following Lymphedema Treatments
Private: Tracking Outcomes Following Lymphedema Treatments
 Private: Microsurgical Procedures: Vascularized Lymph Node Transfer from the Thoracodorsal Axis
Private: Microsurgical Procedures: Vascularized Lymph Node Transfer from the Thoracodorsal Axis
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


