Hypertrichosis
Nathan H. Brewer
I. BACKGROUND
Hypertrichosis is defined as growth of hair on any part of the body in excess of the usual amount expected in a person of similar age, race, and sex.1 Hypertrichosis should not be confused with hirsutism although the treatment options have significant overlap. Hirsutism is the androgendependent growth of hair in a male pattern in a female patient. Hypertrichosis is classified as generalized or localized and may be congenital or acquired. Several hair types may be involved, to include lanugo, vellus, and terminal hair. Hypertrichosis may be an isolated finding or may be associated with an underlying disorder.
Hair plays a significant role in social interaction. Hypertrichosis, if present, is often a stigmatizing factor. The presence of hypertrichosis is not only of cosmetic importance but may also be of medical importance, serving as a clue to internal pathology.
II. CLINICAL PRESENTATION
A. Generalized Hypertrichosis. Generalized hypertrichosis is the presence of increased lanugo, vellus, or terminal hair over a large portion of the body surface. Congenital hypertrichosis lanuginosa is an autosomal dominant disorder manifesting postnatally with diffuse growth of fine silver-gray to blonde lanugo hair which spares only the hands and feet. The lanugo hair may reach lengths greater than 10 cm. Acquired hypertrichosis lanuginosa is the sudden onset of rapidly growing fine lanugo hair over a large surface area. This rare form of generalized hypertrichosis has been reported to herald the presence of an underlying malignancy and has classically been associated with colorectal cancer but also described in association with many other malignancies. Another form of paraneoplastic hypertrichosis with a generalized presentation is POEMS (Polyneuropathy, organomegaly, edema, M-protein, skin abnormalities) syndrome which, in addition to hypertrichosis, presents with peripheral neuropathy, organomegaly, endocrine dysfunction, monoclonal gammopathy, and skin changes. Several drugs are known to cause generalized hypertrichosis (Table 22-1). Several congenital syndromes display generalized hypertrichosis and should be considered when evaluating an infant or young child with generalized hypertrichosis.
B. Localized Hypertrichosis. Localized hypertrichosis has both congenital and acquired forms (Figs. 22-1, 22-2, and 22-3). Becker nevus is a hamartoma, which exhibits hyperpigmentation and hypertrichosis (Fig. 22-4). It has a male predisposition and is typically first noticed in adolescence. Common locations include the shoulders and the upper lateral chest. Nevoid hypertrichosis is characterized as a circumscribed growth of terminal hairs within a patch of normally pigmented skin and without an underlying hamartoma.
TABLE 22-1 Drug-Induced Hypertrichosis | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
 Figure 22-1. Medium-sized congenital melanocytic nevus with hypertrichosis. (With permission from Goodheart HP. Goodheart’s Photoguide of Common Skin Disorders. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2003.) |
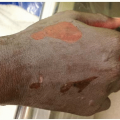
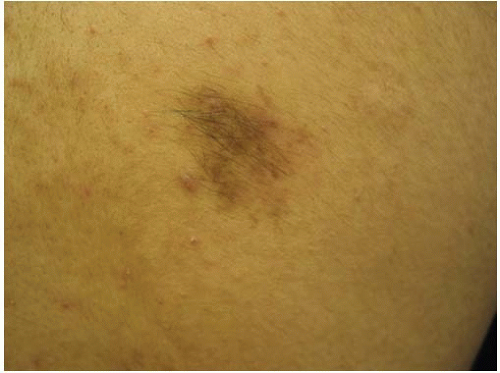 Figure 22-2. Hypertrichosis due to administration of intralesional corticosteroids. (Image provided by Stedman’s.) |
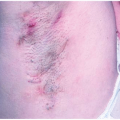
 Figure 22-3. Steroid hypertrichosis. (Image provided by Stedman’s.) |
Inherited forms of hypertrichosis are often localized and frequently have a symmetric distribution (Table 22-2). Localized hypertrichosis following repeated trauma or friction is a well-known entity.
III. WORKUP
Diagnosis of hypertrichosis is dependent on physical examination with characterization of the hair type involved, pattern of hair growth, and age of initial presentation. In addition, physical examination should focus on any associated abnormalities, which may signal the presence of an underlying disorder. Family history and medication history are helpful with diagnosis as well. Biopsy has limited utility in the diagnosis of hypertrichosis. A female patient with hirsutism should be screened for an ovarian or adrenal source of androgen production.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


