Only a few years ago nobody mentioned the term hoodplasty; it did not exist. But thank goodness, today we just cannot conceive of a labiaplasty without also having the option of a hoodplasty. But before we talk more about this procedure, I would like to mention the importance of treating the entire region.
Not liking our genitalia and having an aesthetic genital procedure is no longer something to be ashamed of. Talking about our vagina is not a taboo any more.
Having aesthetic surgery on our genitalia can be simply because we do not like the appearance, which makes us feel uncomfortable when exposed nude to our partner, or can be secondary to functional concerns that can interfere with our day-to-day activities.
These are the reasons patients undergo an aesthetic genital procedure:
They do not like how it looks:
- •
Labia minora too long
- •
Excess skin on the clitoral hood that looks like a penis
- •
Big clitoral gland
- •
Too bulky labia majora that show with the use of tight clothes
- •
Too bulky pubic region that shows through clothes
- •
Empty labia majora
- •
Wrinkled labia majora that make you look older down there
Interferes with their daily activities:
- •
Long labia minora that are pushed inside the vagina during sexual intercourse, making it painful
- •
Long labia minora that pinch when you ride a bike, a horse, etc.
- •
Long labia minora that ulcerate with exercise
- •
Excess skin on clitoral hood that facilitates bad odors
- •
An overexposed clitoral gland
- •
An underexposed clitoral gland
- •
Too little cushion on the pubic area that makes it painful during sexual intercourse
Questions of what is normal in female genital still arise. Many still ask why do surgery in this area? When I listen to these questions, I always think to myself they are being short-sighted. We cannot and must not speak of what is normal in the genital area; every woman is different not only anatomically, but also as to how they perceive their vagina. This is why this procedure, just like any other aesthetic procedure, must be approached in a unique way for each individual patient.
When a labiaplasty is compared with a genital amputation, there is a total misunderstanding of why the procedure is being done. According to the World Heath Organization, a genital amputation is done to limit the woman’s sexual life and decrease enjoyment of her sexuality. By performing a genital aesthetic procedure, what is being done is totally the opposite. When performing any of these aesthetic procedures, we are improving the patient’s quality of life and how she perceives her genital area.
Also, the phrase “they do not know what else to invent,” or “it is just not enough for them to have liposuction and breast augmentation, now they also need to have a procedure done on their genitalia” is synonymous with a person who definitely has not understood the procedure and how important it can be to make one complete. Today, woman are leaders in their families and are also gaining leadership in their jobs. They can be seen as very successful, but still in their sexuality, when they are not comfortable with their genitalia, this can make them feel insecure and prevent them from taking the lead in their intimacy.
Actually, if we only take one thing from this whole chapter, it must be that genital aesthetics is much more than just doing a labiaplasty. When thinking of genital a esthetics, we need to know it is not just one procedure but a group of procedures that will enhance the area.
Also, today we need to know that we can approach the area with surgical and nonsurgical options and this is why it is so important to listen to the patient and understand why she is here with you, asking for an a esthetic genital procedure. This is the only way we can do a correct assessment of the area and end up with the correct treatment plan to be able to have a happy patient.
Surgical aesthetic genital procedures
- •
Labiaplasty
- •
Hoodplasty
- •
Labia majoraplasty
- •
Hymenoplasty
- •
Mons pubis plasty
When talking about the external genital aesthetic surgical procedures, we can decrease labia minora size when they are excessive. Here it is important to understand that labia minora are there for a reason and just cutting them all is not the right approach, because it can bring future problems to the patient, such as an open external introitus and/or a dry vagina. When a labiaplasty is performed on a young woman and labia are cut excessively, usually complications will arise when the woman ages, not while they are young and beautiful. This is why it is very important to talk to the patients and explain why you need to leave some labia minora in the area.
A hoodplasty many times can be done as a complementary procedure to a labiaplasty; it can be done alone or as a secondary procedure when during the initial labiaplasty, this area has been ignored.
Labia majoraplasty can be done to remove excess subcutaneous or fatty tissue. That usually includes also taking away excess on the mons pubis region by liposuction or direct excision. Alternatively, in other patients, the approach can be just the opposite: to increase volume in the labia majora and/or the mons pubis region, usually with fat lipoinjection.
Resection of excess skin on the labia majora can also be done and here it is also important not to take too much skin in patients with excessive looseness on the inner thigh region, or those who have a vagina that is too wide. Taking too much labia majora skin in these patients may result in them ending up with an exposed introitus, which is very difficult to correct afterwards. Also, another key aspect to prevent ending up with an exposed introitus is to never plan the inner border resection of the labia majora into the crease that divides the labia minora and majora or beyond the inner hair line of the labia majora. In patients with dark genital skin, it is important to let them know that a labia majora resection scar can be noticeable.
When the mons pubis is ptotic, lifting of the area can also be done and it is important to calculate the lift well, because when done excessively, it can leave the patient with an exposed clitoral gland that might not be appealing, or worse, that can really bother her when wearing tight clothes.
When a hymenoplasty is required in a patient, it is important to explain that this procedure will only cover the vagina entrance and that it will not tighten her vagina. A hymenoplasty, although a simple procedure that consists of reviving the carunculae remnants and suturing them back together, has a high failure rate. I recommend attempting to do a hymenoplasty only in those patients who have these carunculae remnants and not in those whose carunculae are atrophic.
Nonsurgical aesthetic genital procedures:
- •
G-spot enhancers
- •
Labia majora-enhancing procedures
Labia majora-enhancing procedures can go from using skin-tightening devices such as radiofrequency and lasers to filling the labia majora with hyaluronic acid. Also, skin lightening procedures with depigmentation creams and lasers can be done in this region.
And with G-spot enhancer procedures, it is very important to explain to the patient that these procedures will only expand the area where more sensitivity receptors are located in the anterior vagina wall. If the patient has a loose vagina, they will not work well, since to have sexual gratification with penetration, there is a need to tighten the vagina during sexual intercourse so that the area with more sensitivity receptors, the anterior vagina wall, is impacted. Also, a G-spot enhancer procedure will not change the maximum erogenous zone of that woman. A G-spot enhancer procedure will simply make this woman feel more when she experiences friction on her anterior vagina wall. The G spot, which is more a zone than a spot, is located in the outer anterior vaginal wall behind and up the pubic bone and can be enhanced by applying hyaluronic acid or platelet-rich plasma in the area.
Expert Approach: Hoodplasty
Lina Triana
Plastic Surgeon
Cali, Colombia
Why did you decide to do this technique?
Being a female plastic surgeon, having exposure to aesthetic female patients and giving them the space to really express their concerns gave me the advantage to find out that many of them were uncomfortable with their genital area and just did not know how to express it, or to whom.
This is how I started to become interested in the area to really fulfill these patients’ needs. When researching how to do this better, I mostly found techniques on how to reduce labia minora size, not much more.
When did you learn it or if it is your own, how did you end up doing it?
I started performing labiaplasties back in 2005 by looking at what could be found in the literature but with a particular interest in not just cutting the excess, since I was just not happy with some of my personal cases. I was not really fulfilling what my patients wanted.
I had two main problems:
- 1.
I could not find the right resection technique.
- •
I had patients who just did not like the dark color in their labia minora and when performing the described Alter’s wedge technique, this dark color was not going away.
- •
Performing the edge resection technique took away the dark skin color, but it was easier to end up with a too short labia minora and/or a showing scar.
- •
- 2.
There was something missing in the overall aesthetics, something even after performing the labiaplasty that made some patients (not all) even unhappier. Why was this happening?
By really observing and listening to my patients, I finally started to understand that what made the difference was whether the patient had excess skin on their clitoral hood or not.
Those patients who had a labiaplasty procedure and had no excess on their clitoral hood were happier, so if the problem was arising when there was an excess on this clitoral hood, how could I correct it?
With the wedge resection, I just could not figure out how to correct large excesses. I even worsened their appearance in the attempt to correct it, but I just did not know why. It took me some time to realize that by resecting the wedge, I was lowering the clitoris hood insertion in the labia minora and that worsened the overall appearance. So how I could prevent this from happening? I needed to find a way to relocate the clitoral hood insertion in the labia minora and could not figure out how to do it with the wedge resection. This is why I started migrating to the edge resection technique and then incorporated the longitudinal resection of the clitoral hood to finally end up joining both incisions, and by doing so, being able to relocate the insertion of the clitoral hood into the labia minora wherever I wanted.
In 2007, my journey to empower women with their sexual wellbeing through aesthetic plastic surgery procedures began, and with it the sharing of what I have discovered regarding the clitoral hood.
Can this technique be compared to others and why?
Although we call this a hoodplasty procedure, in the end, it is not just “one technique fits all.” It all started with the longitudinal resection followed by the edge labia minora resection, but today, there are many other ways to resect based on this initial principle that I will share with you.
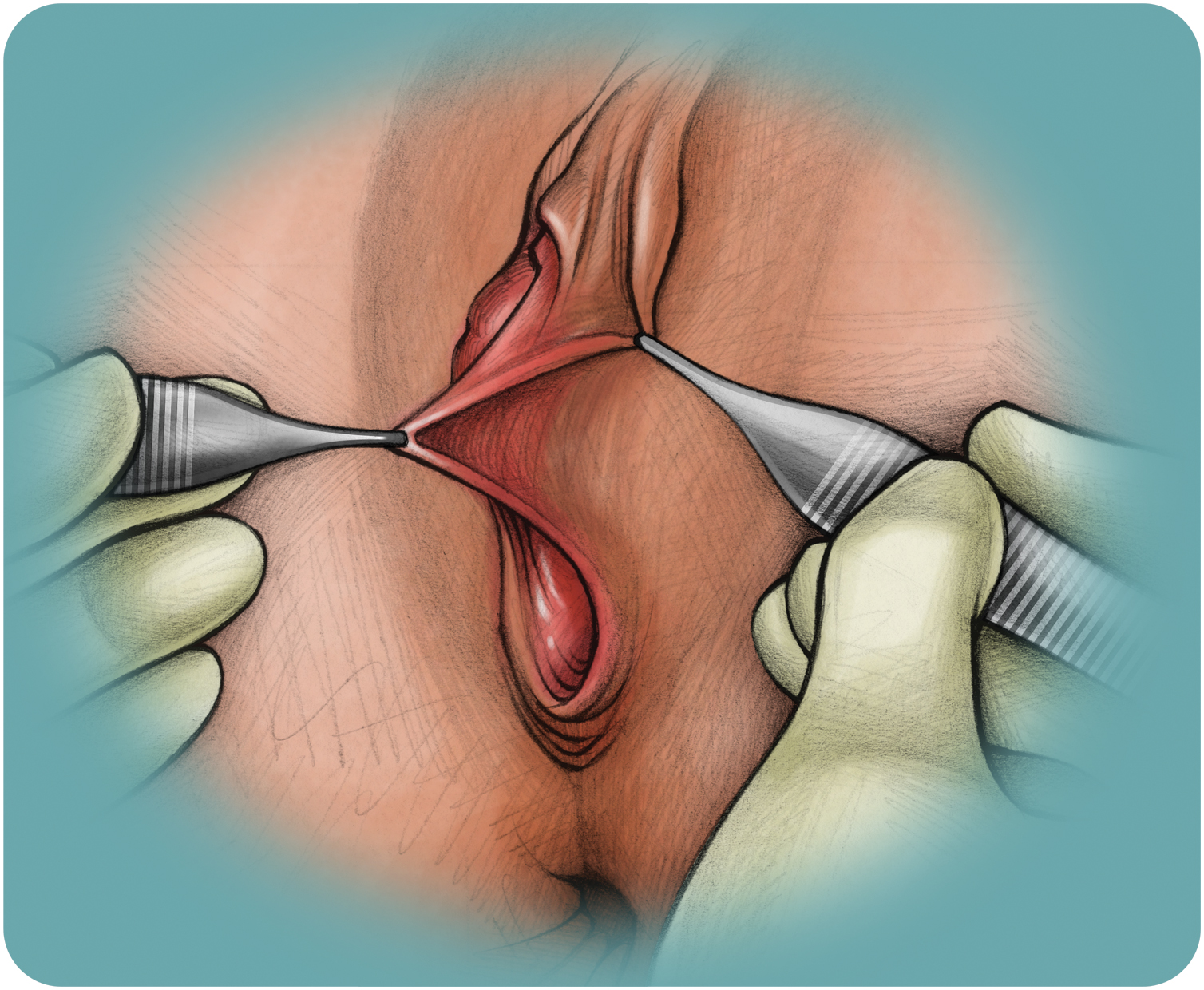
What do you consider to be important landmarks and anatomy to be able to better perform this technique?
To better perform a hoodplasty, it is very important to locate and mark, before we cut or infiltrate the patient, the insertion of the clitoral hood on the labia minora, which is usually not symmetrical, as well as the frenulum.