Just as female genital surgery has been increasing exponentially in the past years, male genital surgery is now becoming more available and with better outcomes, and I am sure that will start increasing also.
Today, more and more men are asking for body definition surgeries and male genital aesthetics serve well to provide a better harmonious figure overall.
Because function is so important, often men were afraid of having these procedures, worrying that in the end they could end up with negative consequences in sexual function, but now we know it is just the opposite. Although the genital aesthetic procedures do not directly improve sexual function in men, from a psychological point of view, feeling more comfortable with their penis length and overall appearance also increases male general confidence.
Penile lengthening procedures as well as increasing the penile girth are generally requested by young adult males who although they do not present with real sexual dysfunction, do feel uncomfortable when referring to their size.
Penile enlargement surgeries can also be included with scrotal procedures for a complete male genital rejuvenation. Just as in women, one must not only talk about one part but the overall male genital aesthetics.
Let’s see what our expert has to tell us. Dr. David Caminer has more than 15 years of experience in the field. While thinking outside the box in ways on how to better serve his patients, he came up with these new modifications to previously described techniques to really impact the overall surgical outcomes in male genital surgery.
Expert Approach to Penile Enlargement: Suspensory Ligament, Fat Grafting, Scrotal Webbing
David Caminer
Plastic Surgeon
Sydney, Australia
Why did you decide to do this technique?
I have been working on my technique for 20 years. I decided to perform this operation the way that I do it so that the complications that I was seeing from others would be minimized. This technique has evolved over the years so I can tell my patients that there will be minimal bad sequelae as a result of the operation. I was seeing some bad complications and it was ruining people’s lives, so I wanted to do a very safe technique.
When did you learn it Or if it is your own, how did you end up doing it?
I learned part of the technique, the division of the suspensory ligament, from urologists, but that is not the complicated part. The issue and the problems that I was seeing were from the fat grafting into the dead space once the suspensory ligament was divided. I felt that filling the dead space with vascularized fat was better than a thick/large piece of nonvascularized fat graft. Just dividing the ligament and not filling the dead space with tissue meant that the scarring would pull the penis up again and the result would be poor. This is the reason historically why penile lengthening by ligament division alone has a very poor reputation.
When I performed a few of these procedures in the area, I noticed quite a lot of fat laterally. I worked out a way to elevate a distally based fat flap and used one from each side to fill the dead space created by the suspensory ligament division.
The other complication I was seeing was related to degloving the penis and using a dermis fat graft as a wrap around the penile shaft for girth augmentation.
Fat grafting worked well for me in other areas with very few complications, so I started to use fat grafting for girth augmentation.
I have been performing this technique for about 15 years now and have found it to be excellent, with very few complications.
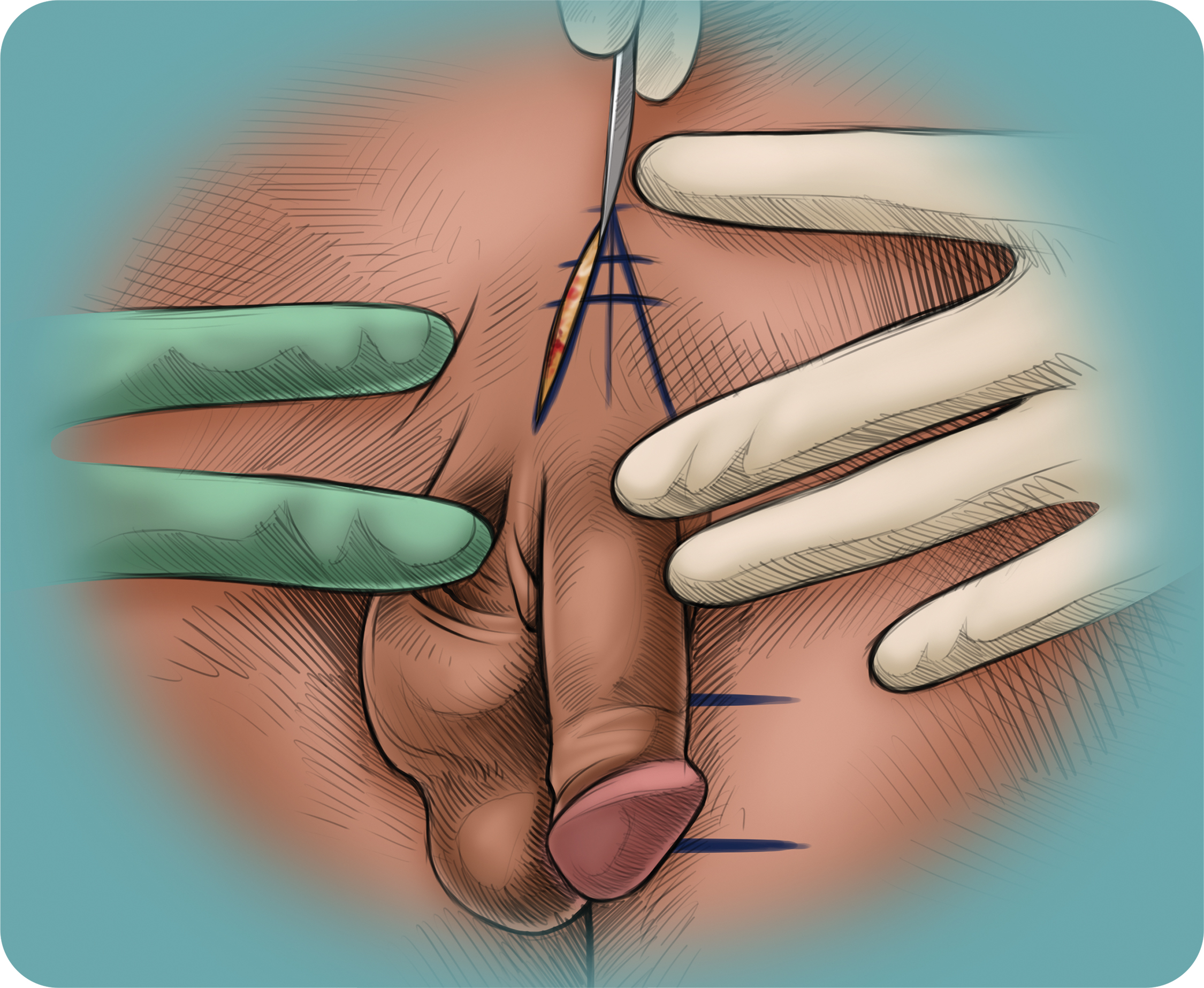
The incision that I perform is for a V–Y advancement flap. This flap has evolved over the last 10 years. At the beginning, I was doing a transverse incision, but I was only getting approximately a maximum of 2 cm increase in length. I was worried about the scar in that area but at some stage, I discussed it with a patient, and he was not worried about the scar if it increased the length gain. I thus decided to do a V–Y advancement flap. The function of this flap is to gain more skin over the proximal penile shaft, which I believe is part of the issue of why penises cannot be extended as much without doing that incision. I have been using this incision in all cases for many years now. I believe that using this V–Y advancement flap incision makes a difference in the final result of the procedure.
Can this technique be compared to others and why?
Yes, this technique can certainly be compared with the other techniques. In all penile lengthening techniques, the suspensory ligament needs to be divided.
How one fills the dead space to keep the penis from retracting back is the difference. This technique can be compared with dermal grafting, but with dermal fat grafting, the problem is with such a big lump of fat, there is often an amount of necrosis that occurs. Whatever necrosis occurs leads to more fibrosis. Fibrosis should be avoided at all costs. Any fibrosis of the penile shaft to the pubis is detrimental for penile length.
The fat flap is a random pedicle vascularized flap. I have not seen any fat necrosis or infection sequelae of these fat flaps. I believe that even in thin people, one can find enough fat tissue in the area to fill this space. Obviously, the fatter the patient is, the more fat there is to harvest. I believe this to be the best scenario. However, if the patient is too fat, his pubic pannus will work against penile length, as it will engulf the penile shaft.
One of the advantages of harvesting fat from the inguinal region and spermatid cord area is that it does make this area less bulky and one can see a flattening of the pubic contour of the area, which many men like.
If people are overweight and need liposuction around the mons pubis area, my recommendation would be that the penile lengthening procedure is performed first. I would not do the liposuction and the penile augmentation at the same time. This is because the area is the most dependent part of the abdomen, leading to prolonged and excessive swelling which delays the healing process. I would stagger the sequence of the liposuction and would recommend that one perform the liposuction at a later stage once the penile lengthening procedure has settled down. I would recommend waiting 4 months before performing liposuction when it is necessary.
My experience with patients who have had liposuction to the pubic area on a prior occasion is that it is usually done on the more central area and does not interfere with the harvesting or the amount of fat that can be harvested from the spermatic cord.
This technique also differs from other techniques of fat grafting of the penile shaft for increased girth.
I am not a fan of dermal fat grafting of the penile shaft. When performing dermal fat grafting of the shaft, one needs to deglove the penis. With any degloving of an organ like this, there is always the possibility of skin necrosis. If, unfortunately, there is a significant amount of skin necrosis in that area, the result is devastating to the patient. I hence stay away from this technique and as such, I think microfat grafting is such a good technique with no chance at all of any skin necrosis of the penile shaft. Other reasons for not liking this technique of dermis fat grafting are the long scars that result from the harvesting of this tissue. There is also the issue of too much bulk at the base of the penis, giving the penis the Eiffel Tower appearance. This is why it is my preferred technique for girth augmentation.
All the articles and myths of lumpiness and no fat take has not been my experience. I harvest the fat as microfat rather than as a normal fat graft with smaller holes in the cannulae. When performing microfat grafting, the contour of the penis is very good and can be adjusted with ease. I do not see any lumpiness.
Fat grafting can be redone if the patient wants further girth increase 6 months after the first procedure.
I do tell the patients they will lose about 50% of the fat. When they wake up, there will have considerable swelling and this does resolve over about 3 weeks. It will take about 4 months to see the final outcome regarding the fat take.
A question that patients often ask is, “Will my penis feel soft?” This does not seem to be a problem. The fat that remains is not such a large amount as to make the penis become soft and boggy. I also believe that with fat grafting, there is certain amount of fibrosis that occurs, and this gives the penis a fairly firm consistency.
What do you consider to be important landmarks and anatomy to be able to better perform this technique?
I think a good understanding of the anatomy of the area is essential. The penile anatomy is not that difficult. One needs to understand that there are the dorsal penile nerves, which is one’s main concern when dividing the ligament. One should stay out of the Buck’s fascia in that area in order to preserve the nerves. This plane is fairly easy to see and to follow down the penile shaft. I dissect as far as the inferior aspect of the pubic symphysis. At this point, the symphysis takes an upward turn, and this is where I stop the dissection. At this point, the neurovascular structures become more at risk of injury.
Other important anatomy is when harvesting the spermatic cord fat flaps, one should understand that any structure in the cord can be divided and understanding the anatomy of the spermatic cord is important. I think the two main structures that worry me are the nerves that travel down in or just adjacent to the cord. I always worry about postoperative long-term pain secondary to nerve injury, as well as numbness. The two nerves in that area are the genital branch of the genital femoral nerve and the ilioinguinal nerve. One must be aware that these structures are nearby, and always be cautious. I prevent injury to them by doing the dissection with loops, and when I visualize the cord, I know that the nerve is nearby. The genital branch of the genitofemoral nerve runs inside the cord and the ilioinguinal branch nerve is outside the cord.
I have never had a patient with any sensory loss of their penis, and I do not believe this technique leads to any erectile problems.
The angle of the erection, I believe, is overstated, and some people believe that when one divides the ligament, the angle of the erection becomes more obtuse. I have not found this to be the case.
Regarding other penile lengthening techniques, some state that you cannot cut all the ligament, as the angle of the erection will be affected. I believe this not to be correct. One can go ahead and divide all the ligament without having significant changes to the angle of the erection.
Can you explain to us how do you do the assessment on a patient asking for this procedure? Can you give us some guidelines for constructing an assessment chart?
The assessment of these patients is pretty simple. They obviously need to have normal penile anatomy, which most men have. What I usually do is to try to make a measurement of the penis. This can be quite variable, depending on numerous factors such as whether the person is cold or frightened. This is mainly for one’s records and to have a comparison postoperatively. A normal penis should be 8–10 cm in the flaccid state and 10–12 cm in the stretched state. I believe I can achieve an increase in length of between 2 and 4 cm. Prospective patients need to know that there may be no lengthening increase, although this is very rare. Another important thing is to assess the fat bulk over the lateral aspect of the mons pubis to give one some idea of the amount of fat in the area for the fat flaps. This is usually not a problem.
One also needs to assess the amount of fat that can be harvested for fat grafting. Any areas are suitable donor sites, but the usual ones are the central abdomen and hips. Very thin people pose a problem for fat grafting, as sometimes there is not enough fat for covering the entire penile girth. I like to inject a minimum of 25 mL of washed fat. If I can only get ∼15 mL, then I only inject the fat over the dorsal surface.
Instead of using fat, one can inject hyaluronic acid (HA) in the same plane as the one used for fat grafting. This can be expensive and is usually used when patients come just for girth increase. The HA is a temporary filler and lasts in the penis for a variable amount of time. Men do not need to have a general anesthetic for this, and they will not need to go to the operating room for HA injections. When HA is used, I recommend using it in the penile shaft only. I do not inject the glans penis with fat or HA, as over the glans there is no plane to inject as there is over the penile shaft. The skin over the glans is firmly adherent to the deep fascia. I perform HA injections for the penile shaft in my office under a dorsal penile block.
There are no differences whether the penis is circumcised or not. I perform the same operation in both, although the fat grafting of the foreskin is a little bit more problematic. One needs to be quite conservative in putting a lot of fat into the foreskin. I found that because the skin is quite thin and there are two layers of this thin skin over this area that one can get some unevenness of the contour in the foreskin. One thus needs to be quite careful when putting fat into the foreskin. I also find that fat take seems to be less in the foreskin than around the shaft.
Can you describe your technique?
My technique starts with the division of the suspension ligament.
I like to do the lengthening part first and this I do by designing a distally based V–Y advancement flap with the wide edges of the V being on each side of the proximal part of the dorsal penis shaft.