Why Did You Decide to Do This Technique?
Penis enlargement is becoming more popular every day and thousands of male individuals are seeking some help to satisfy their desire.
Our community, however, is generally skeptical of performing penile enlargements because of the uncertain results and bad reputation, mostly produced by non-board-certified plastic surgeon physicians or unprepared medical professionals and commercial agencies, who reproduce and imitate the penis enlargement surgical procedure. Many individuals have ended up dissatisfied, with severe complications, because they have been offered paramedical, practical, surgical, or nonsurgical therapies and have been cheated with treatment options without a doubt are not in the armamentarium of any ethical plastic surgeon or even respectful physician.
We never put any pressure on an individual to proceed with this operation. It is his sovereign decision whether to proceed or not. We should never promise results that surpass the capability of our technique. Patients with unrealistic expectations, who request results superior to those explained, or who feel entitled to obtain the maximum penile increase based on ideas and perceptions coming from adult videos, should be excluded.
But before we start analyzing the plastic surgery methods that enhance penis enlargement, we need to review the physiological function and size of the penis, the history, anatomy, and histology for this operation.
When Did You Learn It? Historically, What Is Your Contribution?
In 1982, a French plastic surgeon, Yve Gerard Ylouz, was probably the first to liporecycle fat microparticles (lipoaspirates), for cosmetic purposes. That was performed on a young actress, a close friend of Ylouz, by aspirating the fat cells of a lipoma on her back, using a very small liposuction cannula and transferring the lipoaspirate as it was, to the deep nasolabial folds. I was present as an assistant young plastic surgeon at this historical procedure and at many more to follow, evaluating and developing the lipotransfer technique. We used the term liporecycling, interpreted from the Greek Λίπο ανακύκλωση (leapo anakeekclossi) , meaning literally recycling the fat. In 1983, at the BAAPS course in London, together with Bryan Mayou, we presented officially ( ISAPS Newsletter, September–December 2012, 27–29), maybe the first in the UK, the new technique of liposuction and a few years later, lipotransfer of lipoaspirates. After that year, liporecycling became maybe the most wanted, frequent, and popular plastic surgery procedure and ever since, plastic surgeons all over the world have reliably used fat grafting as a way to improve and enhance cosmetic appearance or augment many anatomical areas. Either as a core procedure or an adjunct to several other plastic reconstructive or cosmetic surgery procedures on breast, face, scalp, feet, hands, hips, buttocks, and endless other anatomical sites, today liporecycling remains within the top five plastic surgery procedures.
Two major disappointment in those early years was that the transplanted fat was short surviving and that the fat could not be preserved for later second-time use. Over the last 15–20 years, plastic surgeons started, and then clinicians followed, to document in several publications the therapeutic benefits of fat grafting with or without added platelet-rich plasma (PRP) and adipose tissue-derived stem cells (ATSCs, which are present of course in the stromal vascular fraction, [SVF]).
Given today’s answers and knowledge, during that time of the late ’70s and early ’80s, fat recycling was the subject of extended studies and strong discussions, and considered the hot topic for congresses and scientific panels. As well, at the same time, as plastic surgeons, we received vast amounts of ironic comments and dispute, unfortunately not only from other physicians, but sadly from conservative or skeptical members of our own society.
Nowadays, many other non-plastic surgery specialties are using liporecycling to assist their procedures and enhance their therapeutic results. Gynecology, orthopedics, urology, ophthalmic surgery, ENT, dermatology, and of course, general surgery are among those specialties using fat in addition to the most commonly done plastic surgries.
In fat-grafting history, we see the names of Gustav Neuber (1850–1932 German plastic surgeon) and Dr. Viktor Czerny, a German Bohemian surgeon, who at the beginning of the early 20th century used lipografting not as harvested fat micro lipoaspirates, but as an entire lipoma or a fat-piece transfer. In fact, fat grafting at the beginning indeed had trouble gaining acceptance, mainly for its poor results, as modern liposuction techniques had not yet been developed or standardized, and there was a lack of experience and knowledge.
Fat grafting should be performed in a hospital or outpatient surgery center, and when done in private consultation facilities, only as where they are accredited. Facility accreditation is important as it guarantees that the specific facility is inspected at regular intervals by the public health authorities or ministry, ensuring patient safety, best practices, and that operations are performed by certified plastic surgeons.
Can This Technique Be Compared To Others and Why?
Surgical penis enlargement and elongation methods include various types of penile augmentation and suspensory ligament release. Penile augmentation involves injecting mostly fat cells or other types of injectables into the penis, or grafting dermofat pieces. Injecting fat cells into the penis is the most common technique.
When done by inexperienced physicians, fat transfer, fillers injection, and placing dermo-fat grafts into the penis (usually to the dorsum) can cause severe deformity and functional issues, which, in some instances, are long-lasting or unrepairable. Suspensory ligament surgery produces a high rate of functional issues. All those surgeries leave scarring at the operation and donor site and the results in size may disappear over a short time, leaving calcified tissue. For the recipient individual, this is a most uncomfortable and unpleasant situation that demands extrusion and correction, which sometimes is not very successful.
Suspensory ligament release increases flaccid penis length, but does not increase by any means the length of an erect penis and usually because of the instability that this operation produces, creates firmness problems with sexual dysfunction. The suspensory ligament is the remainder in mankind of the erectile bone in canids (dogs, wolves, and many more carnivores, household or wild). Functionally, the suspensory ligament supports and maintains the base of the penis attached to the pubis. It is the main point of support and straightening for the erect penis, keeping it in an upright and stable position during sexual intercourse.
Expert Approach: Fat Grafting to the Penis
Theodore Vodoukis
Plastic Surgeon
Athens, Greece
How did you end up doing it?
We must emphasize that the initiative of this study was to assist plastic surgeons when counseling patients considering or asking for penile cosmetic surgery (for length and circumference augmentation) and to provide them with guidelines on the technique to perform the best possible operation and obtain optimum results.
Can this technique be compared to others and why?
There are several surgical or nonsurgical penis enlargement treatments, most of which carry a risk of significant complications and give no results, especially when performed by unlicensed physicians, which can lead to disaster.
The American Urological Association (AUA) and the Urology Care Foundation “consider subcutaneous fat injection for increasing penile girth to be a procedure which has not been shown to be safe or efficacious. The AUA also considers the division of the suspensory ligament of the penis for increasing penile length in adults to be a procedure which has not been shown to be safe or efficacious.” Also, complications from penis enlargement procedures using dermo-fat, are the worst, including scarring that may lead, eventually, to penis shrinkage or erectile dysfunction.
Other surgical treatments include the injection of dermal fillers, silicone gel, or poly(methyl methacrylate)—PMMA. All those methods are also not approved, not only by the US Food and Drug Administration (FDA) for use in the penis, but also are mostly refused by serious professionals.
A 2019 study in Sexual Medicine Reviews found that nonsurgical methods of penis enlargement are typically ineffective and can be damaging to both physical and mental health. The authors found that such treatments are “supported by scant, low-quality evidence, unethical advertisement, fake statistics, news and rumors.”
Injectable pharmacological drugs (papaverine) and fat transfer surgery should remain the best options, considered as the only ethical procedures, and all others should remain in clinical trials.
Again, according to the 2019 study in Sexual Medical Reviews, Överall, other treatments’ outcomes performed by non-specialized physicians, were from little acceptance to poor, with low satisfaction rates and significant risk of major complications, including penile deformity, shortening, and erectile dysfunction.”
Without commenting on those reviews, even if they are coming from the most reputable entities, we will concentrate on the plastic surgery options, as plastic surgery is the core knowledge in the area of penis enlargement. Offering the most advanced combined techniques of fat transfer, that really have changed the results and statistics, posturing acceptable long-lasting results, cover the up to now lack of a reliable method for this operation.
Fat transfer or liporecycling for penis enlargement (also referred to as fat grafting or fat injections), is the surgical process by which fat is harvested and implanted from one area of the body to the penis of the same individual. The objective is to augment, correct, or support the area where the fat is injected. The technique involves extracting adipose fat by means of mini-liposuction, processing the fat in-house (international regulations prohibit the transport of collected fat outside of the surgery premises for further processing), and then reinjecting it into the penis. We have concluded that injecting fat together with PRP, fat tissue stem cells (FTSCs), which exist mostly in the SVF, all prepared at the same time in the operating theater, gives much better and longer-lasting results, contradicting the theory of a nonviable operation.
What do you consider to be important landmarks and anatomy to be able to better perform this technique?
Histology
Fat tissue consists of three main types of fat or adipose cells. An average human adult has 30 billion fat cells with a weight of 30 pounds, or 13.5 kg. If excess weight is gained as an adult, fat cells increase in size about fourfold before dividing and increasing the absolute number of fat cells present. Of major importance is the fact that the proportion of volume to weight of fat is not 1:1. One cubic centimeter of fat weighs 0.7–0.8 g.
White Fat Cells (Unilocular Cells)
A typical fat cell is 0.1 mm in diameter, with some being twice that size and others half that size. White fat cells contain a large lipid droplet surrounded by a layer of cytoplasm. The nucleus is flattened and located on the periphery. The fat stored is in a semiliquid state and is composed primarily of triglycerides and cholesteryl ester. White fat cells secrete many proteins acting as adipokines, such as resistin, adiponectin, leptin, and apelin.
Brown Fat Cells (Multilocular Cells)
These are polyhedral in shape. Unlike white fat cells, these cells have considerable cytoplasm, with lipid droplets scattered throughout. The nucleus is round, and, although eccentrically located, it is not in the periphery of the cell. The brown color comes from a large number of mitochondria. Brown fat, also known as “baby fat,” is used to generate energy in several forms.
Marrow Fat Cells (Unilocular Cells)
Marrow adipocytes, like brown and white adipocytes, are derived from mesenchymal stem cells.
The marrow adipose tissue deposit is poorly understood in terms of its physiologic function and relevance to bone health. Marrow adipose tissue expands in situations of low bone density, but additionally, it expands in the setting of obesity.
Since the new millennium, several groups of plastic surgeons and researchers from all over the world have already published many papers on tissue engineering, describing the implications and assistance of adipose tissue in the new cell-based regenerative therapies. This was quite a revelation and at the same time a relief to the scientific community, as up until the last century, adult mesenchymal stem cells (MSCs) were thought to exist predominantly as a bone marrow product. As it turns out in the last decades, adipose tissue is a much more rich, perpetual, and prolific source of MSCs than bone marrow. By volume, MSCs are actually 300–500 times more plentiful in adipose tissue as compared with bone marrow tissue. Together with the ease of harvesting and extraction of adipose tissue (compared with bone marrow), this opened up a whole new chapter in the field of reconstructive and regenerative plastic surgery.
A Normal or Acceptable Size for the Penis
Although results vary slightly across reputable studies, the accepted mean for the human penis, when erect, varies within the range of 12.9–15 cm (5.1–5.9 in) in length. It is not necessarily correlated with anthropometric measurements such as height, weight, and body mass index (BMI).
In a systematic review published in the International British Journal of Urology by , covering the previous 30 years research on the topic, they presented data showing almost similar results, giving mean penis lengths when flaccid of 9.16 cm, stretched nonerect of 13.24 cm, and erect of 13.12 cm respectively, and mean flaccid or erect circumferences (girth) of 9.31 cm and 11.66 cm respectively.
The most important factor that affects penile dimensions, beyond any doubt or skepticism, is the arousal and the frequency of arousal during every man’s whole life. Sexual arousal, also called sexual excitement or desire, is typically and literally what men want during or in anticipation and expectancy of sexual activity. A number of physiological reactions occur mainly in the mind and consecutively to the body as preparation for sexual intercourse and continue during it. Male arousal will lead under any circumstances to an erection; that is a simple biological pattern. The female arousal response involves sexual tissues such as nipples, vulva, clitoris, vaginal walls, and vaginal lubrication, having a more complicated pattern. Mental and physical stimuli such as touch, odor, view, and the internal fluctuation of hormones influence and maintain sexual arousal. Sexual arousal has several stages and may not lead always to any actual sexual activity, apart from mental arousal and the physiological changes that come with it. Given sufficient sexual stimulation, sexual arousal in humans reaches its climax during an orgasm. It may also be pursued for its own sake, even in the absence of an orgasm, especially for youngsters.
However, the relationship between erection and arousal is not one-to-one. After their mid-fifties (depending as well on the culture of the individual), men report that they do not always have an erection when they are sexually aroused or challenged.
Length When Flaccid
The length of the flaccid penis does not necessarily mirror the length of the erect penis; some smaller flaccid penises become much longer, whereas some larger flaccid penises show comparatively less elongation.
Owing to the action of the complex cremaster muscle-ligament, the penis and scrotum can contract involuntarily in response to cold temperatures, fear, nervousness, and anxiety, referred to by the slang term “shrinkage.” The same phenomenon affects men who sit all day during their jobs, drivers, cyclists, and exercise bike users who receive prolonged pressure on the perineum from the chair, driving seat, bicycle, or saddle. The lack of exercise, movement, or standing causes the penis and scrotum to contract involuntarily. An incorrect seat or long sitting in a saddle may eventually cause erectile dysfunction.
Length When Stretched
In 2015, a study of 15,521 men found that the average length of a stretched flaccid penis was 13.24 cm (5.21 inches) long. This is nearly indistinguishable from the average length of an erect human penis, which is 13.12 cm (5.17 inches) long, meaning that more or less, a stretched flaccid penis only changes in girth when erect.
Neither age, ethnicity, or size of the flaccid penis could accurately foresee erectile length. But stretched (when flaccid) length has a notable correlation with erect length, although we have not seen drastic differences between stretched and erect lengths.
An Italian study of around 3300 men published in European Urology concluded that flaccid stretched length on average measured about 12.5 cm (4.9 in), while an erect human penis is 13.12 cm (5.17 inches) long. In addition, when they checked for correlations in a random group of the same sample consisting of 325 men, they found statistically a very slight linear correlation (Spearman). Significant correlations exist between flaccid length and height of -0.208, weight -0.140, and -0.238 with BMI (flaccid circumference and height of -0.156, -stretched length and height -0.221, weight -0.136, BMI -0.169). As Spearman’s correlation is NOT a linear one, we do not expect that a man with a high BMI to always have a relatively bigger and wider penis.
In statistics, Spearman’s rank correlation coefficient, denoted by the Greek letter ρ (rho), is a nonparametric measure of rank correlation (statistical dependence between the rankings of two variables).
When Erect
Studies relying on self-measurement, including those from Internet surveys, consistently reported a higher average length than those using medical or scientific methods to obtain measurements. This emphasizes and provides evidence here of the personal psychological factor, self-esteem, and individual’s point of view.
In a study of 80 healthy males, the average erect penis length was measured as 12.9 cm (5.1 in) ( Journal of Urology , September 1996). Erection was pharmacologically induced in 80 physically normal American men (varying ethnicity, average age 54). It was concluded: “Neither patient age nor size of the flaccid penis can accurately predict erectile length.”
A review published in the 2007 issue of BJU International showed the average erect penis length to be 14–16 cm (5.5–6.3 in) and girth to be 12–13 cm (4.7–5.1 in). The paper compared the results of 12 studies conducted on different populations in several countries.
An Indian study of 500 men aged 18–60 published in the International Journal of Impotence Research found, respectively, length to be: flaccid, 8.21 cm (3.23 in); stretched, 10.88 cm (4.28 in); and erect, 13.01 cm (5.12 in).
The most recent Korean study (published in 2016) of 248 Korean men identified the average erect penile length to be 13.53 cm (5.33 in).
All these citations are mentioned here to emphasize the fact of similarity in the penis dimensions, regardless of country, race, or other anthropomorphic values.
Can you explain to us how you do the assessment on a patient asking for this procedure?
It is not ethical or scientifically advisable, even against the physician’s reputation, to proceed with penis enlargement to individuals suffering from diabetes, immunology and collagen diseases, coagulopathies, cardiopathies, neoplasia, individuals under chemoradiotherapy, infections in progress, those who had prior pelvic surgeries for urogenital conditions or trauma, severe systemic conditions, significant anxiety, distorted or not accepting of their sex (gender dysphoria needs entirely another plastic surgery approach), not accepting of their body image, with history of suicidal thoughts and/or attempted suicide linked to presumed genital inadequacy with psychogenic sexual dysfunction and psychiatric conditions under treatment.
Cases as well of true hypoplasia (micropenis), defined as a length of <2.5 cm relaxed, should follow another pathway of surveys and possible treatment.
It is an absolute contraindication to fat transfer patients taking immunosuppressive medications.
There are two types of individuals presenting in our offices seeking a procedure to have their penis surgically augmented:
- (A)
Those who are having really objective problems in size and girth based on reasonable reasons such as congenital, trauma, postsurgical complications, and time- and age-related conditions at the inconvenient moment (temperature, nervousness, and anxiety or psychological status).
- (B)
Men who have a normal-sized penis or even bigger, but who may experience penile dysmorphophobia by underestimating their own penis size while overestimating others’ average penis size. Such dysmorphophobia is enhanced these days by the widely available circulation of pornographic movies mainly on the Web, showing extra-gifted individuals participating in those kinds of videos, but usually having pharmaceutically or technically induced big erect genitalia, rather than being a gifted man.
Both of those categories involve individuals who already have visited nonmedical professionals, asking for, or even having already had, surgical procedures, technical aids, or pharmacological treatments without, of course, getting any results. All those are mostly guided by fake scam advertisements.
Can you describe your technique?
Penis Enlargement by Fat Grafting Process
It is strongly advisable that the individual’s medical history be fully gathered and medical examination and tests are done (routine blood tests, X-ray, cardio), including an objective examination of the external genitalia, photos, and measurement of the length and circumference of the penis at rest (flaccid) and stretched. It is advisable to do a basal penile ultrasound scan to verify the presence of nodules, plaques, or lesions in the internal tissues of the penis.
PRP Preparation
Centrifugation: The Earth’s gravitational force is sufficient to separate many types of particles if a substance remains motionless for several minutes. A tube of an anticoagulated blood sample left standing still on a benchtop will eventually separate into red blood cell (RBC) and white blood cell (WBC) fractions and plasma. However, the time required excludes this method of separation for most applications in the operating theater. In addition, the actual degradation of biological compounds during prolonged storage demands faster segmentation and separation techniques. Thus, to quicken sedimentation, the effect of gravity is amplified using centrifugal force, which can represent many thousand times the force of gravity.
We prefer to use the centrifuge PRP preparation method, as it is more economical, reliable, and quick.
We obtain a blood sample by venipuncture in acid citrate dextrose (ACD) tubes, a total of 30–40 mL.
Do not chill the blood at any time before or during platelet separation.
Centrifuge the blood using a “soft spin”; 300 rev/min for 6 minutes.
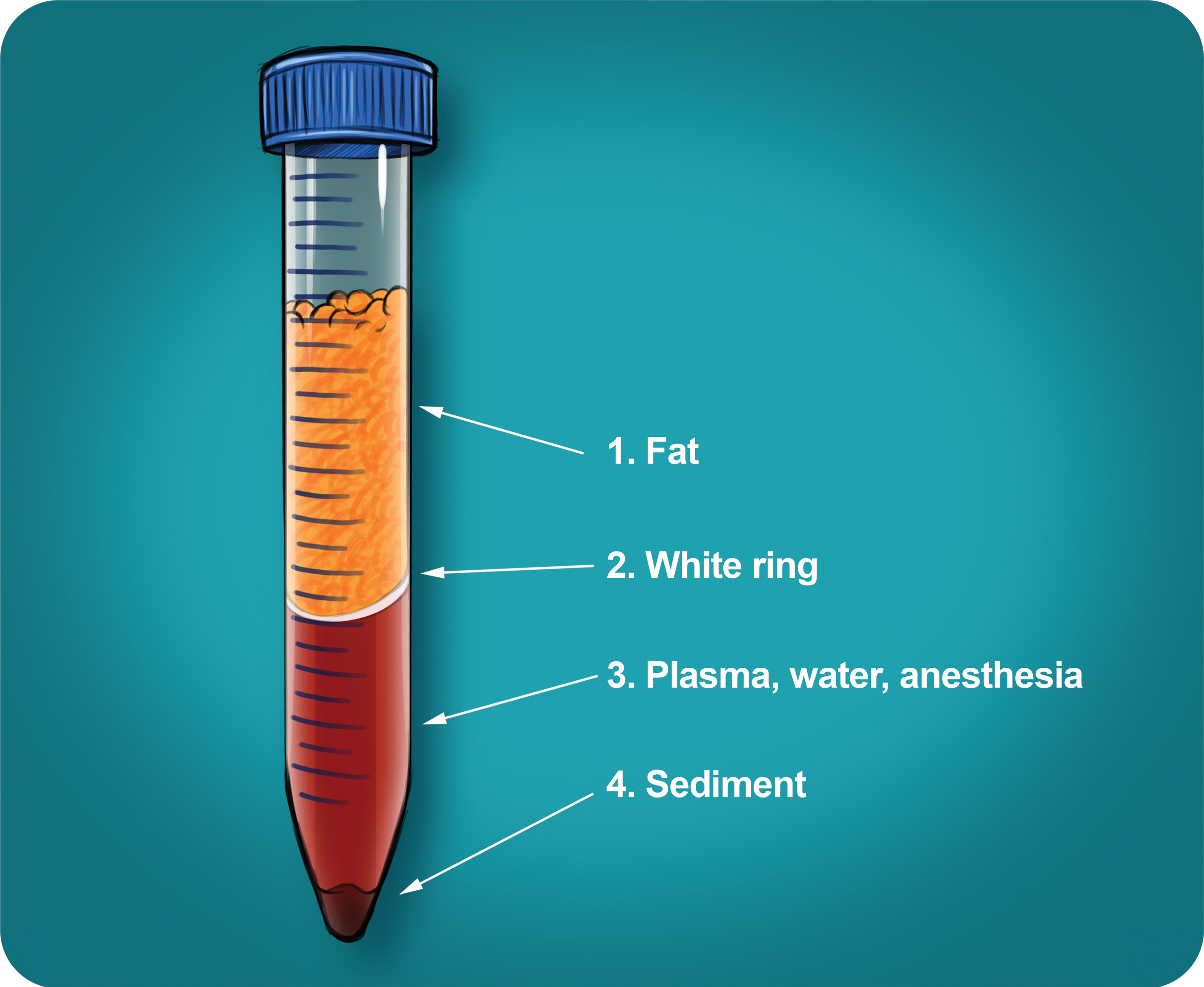
Three layers are separated because of different densities: the bottom layer consisting of RBCs, the middle layer consisting of platelets and WBCs, and the top the platelet-poor plasma (PPP) layer. The PPP layer should be collected and aseptically stored to be used to dilute the SVF later.
Transfer the middle section plasma, as it is the part that contains some platelets, into another sterile tube (without anticoagulant).
Centrifuge the tube at a higher speed (a hard spin) of 600 rev/min for at least 12 minutes to obtain a platelet concentrate.
The lower two thirds is the PRP and the upper third is again the remaining PPP that should be removed and stored with the first one. At the bottom of the tube, a dense pellet is formed.
Remove the PRP and carefully mix the remaining pellet with the preserved and stored aside PPP quantity of plasma (4–8 mL) by gently shaking the tube.
The layer of PRP prepared by centrifugation will be injected equally subcutaneously to the whole shaft surface, acting as a tissue separator (in between the skin and loose circumferential tissue and superficial and deep fascia layers), but mostly acting as a nutrient for the injected fat graft. The PPP will be used to dilute the SVF.
SVF (ATSCs) Preparation
It is emphasized that the preparation of all the endogenic factors should be done within the operating area where the fat and blood is collected. This is because of the international guidance and rules that apply to most countries: If any of the harvested fat or blood leaves the accredited operation theater area to be manipulated or processed elsewhere, it should be considered furthermore not as a surgical homogenous tool to complete the operation, but will enter the regulations as a prepared medication, subject to all pharmacological rules and approval.
Here there is a controversy. Surgical standards based upon a single operation on a single patient in an accredited operation theater differ significantly and by all means are higher than those from the Good Manufacturing Practices (GMP) standards, enforced in commercial pharmaceutical laboratories or companies for mass-produced pharmaceuticals. However, any manufactured drug is required at the end of the production line to be identical in constituents, purity, dose, strength, and be in mass production, whereas autologous SVF could never be produced and characterized that way. Every “amount” of produced SVF is individual, like its individual donor. The guarantee for higher standards of the in-theater–produced SVF than those of an drug manufactured under GMP is also a matter of an accordingly equipped laboratory. Within the sterile area of the operating theater and, of course, with the aid of well-trained personnel (biologists, biochemists, or paramedics) who are qualified to produce on-site (with the necessary equipment) the absolutely essential materials for the transfer—PRP, SVF, ADSCs—the absolute highest quality of the product is indisputable. And, of course, this automatically comes under the domain of the plastic surgeon to produce and deploy the cells for their patient’s benefit for a successful penis fat transfer.
In the vast majority of medical works, it is noted that the adipose tissue, or fat, is the source of SVF, but the truth is that it is not the adipose tissue, only the stromal part of the fat obtained in lipoaspirates (Greek στρώμα, “stroma,” which means the layer, thereafter here the layers of loose connective tissue). Histologically, the fat lobules are encircled by loose connective tissue (stromal) and the SVF cells are present only in the loose connective tissue, which is also the home of capillaries and small vessels and not the fat tissue. Stromal tissue is a widely used histological term referring to loose connective tissue.