Chapter 29 High-Stiffness, Slippage-Resistant Cortical Fixation Has Many Advantages over Intratunnel Fixation
Fixation Stiffness and Slippage: Critical Factors in Restoring Anterior Laxity
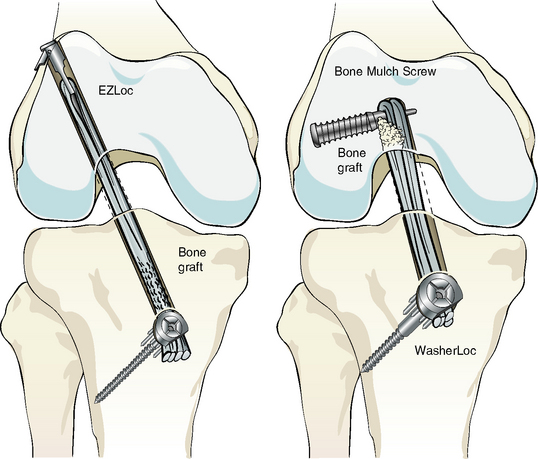
An ACL graft construct is composed of the ACL graft and the two fixation devices at either end (Fig. 29-1). Anterior laxity in the knee of the athlete returning to sport is determined by the stiffness of the ACL graft construct and the length of the ACL graft, not by the strength of the graft and the tension in the graft.1–4
The stiffness of the ACL graft construct determines anterior laxity, the firmness of the Lachman test, and the quality of the “endpoint.” The stiffness of the ACL graft construct is increased more by the use of stiffer fixation devices than by the use of a shorter graft. A short graft with elastic fixation does not restore anterior laxity as well as a longer graft with stiffer fixation.5,6 The concept that shortening the graft increases the stiffness of the ACL graft construct, as proposed by some studies,7–9 is incorrect when high-stiffness, slippage-resistant cortical fixation devices are used.4 The most effective way to construct a stiff ACL graft and restore a firm Lachman test is to use high-stiffness, slippage-resistant cortical fixation devices on both ends of the graft.1,3,5,6
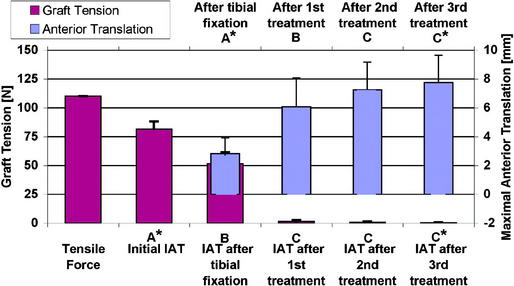
A determinant of anterior laxity that is as equally determinant as the stiffness of the ACL graft construct is maintenance of the length of the ACL graft set at the time of fixation. Maintaining the initial set length of the ACL graft after implantation requires the use of fixation devices that resist slippage during cyclical loading and exercise. Fortunately, there are fixation devices that do resist slippage and provide high stiffness; however, they are applied at the distal end of the tunnels and engage cortical bone, which is 30 times stronger than cancellous bone.5,10–12 The use of intratunnel devices such as the interference screw and IntraFix (DePuy Mitek, Norwood, MA) do not resist slippage, and the ACL graft readily elongates under cyclical load.5,13–15 Therefore the use of high-stiffness, slippage-resistant cortical fixation that purchases cortical bone is the best strategy for maintaining the initial length of the ACL graft and compensating for the obligatory loss in tension from cyclical movement of the knee and exercise (Fig. 29-2).2,3
Definition and Examples of High- and Low-Stiffness Fixation
High-stiffness fixation can be arbitrarily defined as a fixation stiffness that is greater than 400 N/mm when tested in young human bone. The WasherLoc with bone dowel (stiffness of 565 N/mm), the WasherLoc alone (506 N/mm), and tandem screws and washers placed on the cortex distal to the tibial tunnel (414 N/mm) all provide stiffness greater than 400 N/mm in young human bone (see Fig. 29-1). On the femoral side, the EZLoc (infinite stiffness) and Bone Mulch Screw (575 N/mm) are high-stiffness fixations because they purchase cortical bone, which is 30 times stronger than cancellous bone. Each of these high-stiffness cortical fixation devices resists slippage well during cyclical loading.5,6,11,16–20
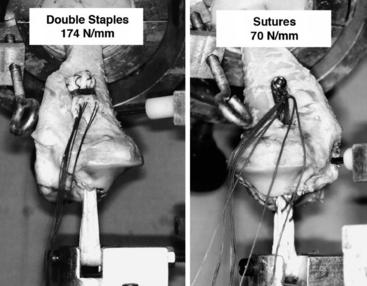
In contrast, low-stiffness fixation provides less than 400 N/mm in young human bone (Fig. 29-3). The interference screw (340 N/mm), double staples placed in the cortex distal to the tibial tunnel (174 N/mm), sutures tied to a post (70 N/mm), closed loop Endobutton (79 N/mm), IntraFix (49 N/mm), and sutures tied to an Endobutton (25 N/mm) are all examples of fixation devices that provide low stiffness. None of these low-stiffness intratunnel and cortical fixation devices resists slippage well during cyclical loading.*
Comment About Intratunnel Fixation with an Interference Screw
The location of fixation of an ACL graft with respect to the joint line has been a topic of debate.17,22–24 Proponents of fixation of an ACL graft at the level of the joint line with an interference screw base their opinion on two studies.7,9 The seminal study showed that anterior laxity was better restored with intratunnel fixation with an interference screw than with double staples applied distal to the tibial tunnel in porcine knees.7 A subsequent study showed that anterior laxity was better restored with intratunnel fixation with an interference screw than with sutures tied to a post in human knees.9 The explanation offered for the better restoration of anterior laxity with intratunnel fixation with an interference screw versus cortical fixation with double staples and sutures tied to a post was that intratunnel fixation shortens the effective length of the graft, which increases the stiffness of the knee.7–9
More recent studies have questioned the use of double staples, sutures tied to a post, and porcine knees to study the effect of the level of fixation on anterior laxity and knee stiffness. Double staples (174 N/mm) and sutures tied to a post (70 N/mm) are low-stiffness fixation devices (i.e., <200 N/mm), whereas distal tibial fixation devices such as tandem screws and washers (414 N/mm), WasherLoc (506 N/mm), and WasherLoc and bone dowel (565 N/mm) are high-stiffness fixation devices (i.e., >400 N/mm).5,17
Related posts:
 Anatomical Anterior Cruciate Ligament Reconstruction with Double-Bundle, Double-Stranded Hamstring Autografts: A Four-Tunnel Technique
Anatomical Anterior Cruciate Ligament Reconstruction with Double-Bundle, Double-Stranded Hamstring Autografts: A Four-Tunnel Technique
 Tibial Fixation for Anterior Cruciate Ligament Hamstring Grafts: 10 Techniques that Improve Fixation
Tibial Fixation for Anterior Cruciate Ligament Hamstring Grafts: 10 Techniques that Improve Fixation
 Hamstring Regeneration Following Harvest for Anterior Cruciate Ligament Reconstruction: A Review of the Current Literature
Hamstring Regeneration Following Harvest for Anterior Cruciate Ligament Reconstruction: A Review of the Current Literature
 Anatomical Double-Bundle Reconstruction of the Anterior Cruciate Ligament
Anatomical Double-Bundle Reconstruction of the Anterior Cruciate Ligament
 Stiffness: Prevention and Treatment
Stiffness: Prevention and Treatment
 Endobutton Anterior Cruciate Ligament Reconstruction Femoral Fixation
Endobutton Anterior Cruciate Ligament Reconstruction Femoral Fixation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


