Chapter 25 High lateral tension abdominoplasty
• The high lateral tension abdominoplasty rejuvenates not just the anterior abdomen, but also the inguinal region, proximal thighs, mons, buttocks, and even posture.
• There is only undermining where skin will be excised or for plication, thereby permitting simultaneous liposuction. Tension is reduced on the mons with less central excision, and the greatest load is carried on the lateral limbs of the incision, thereby increasing the frequency at which the umbilical site will not be closed. The incision will be longer, and the lateral portions of the incision will rise obliquely more than with a traditional abdominoplasty.
• Abdomens differ and since final tension can only be felt intraoperatively, there is no diagram that can demonstrate exactly how to mark either the initial or the final incision. The surgeon must understand the distinguishing principles of this approach and apply them to each patient individually.
• An abdominoplasty is an entirely elective, cosmetic procedure. However, DVT, PE, and even death can occur. Their incidence can be reduced but not eliminated.
• Patients’ primary objections are the location, length, and width of the scars. This should be a major focus during the preoperative discussion with the patient.
 For additional online content vist http://www.expertconsult.com
For additional online content vist http://www.expertconsult.com
Introduction
The high lateral tension abdominoplasty (HLT) accomplishes far more than a flatter anterior abdomen: it is a modified lower body lifting procedure. Lockwood1 noted that his body lifting procedure improved the abdomen more than did an abdominoplasty. He attributed this to his observation that the greatest laxity is lateral, and therefore a greater amount of excision should occur in those areas (Table 25.1).
TABLE 25.1 Comparison of HLT to Standard Abdominoplasty
| HLT | Standard | |
|---|---|---|
| Objective | Rejuvenation of abdomen and trunk | Rejuvenation of central abdomen |
| Anatomical basis | Greatest laxity is lateral | Greatest laxity is central |
| Incision | Lower centrally, raising laterally obliquely, usually longer | More superior and horizontal, usually shorter |
| Umbilicus management | Better to close site vertically than to pull tighter to excise | Better to pull tighter to excise than to close vertically |
| Areas of improvement | Central abdomen as well as flanks, inguinal region, buttocks | Mostly central abdomen |
| Simultaneous liposuction | Can be more liberal | Should be more reserved |
| Location of tension | Greatest tension on lateral limbs of incision along inguinal crease; less tension centrally on the mons | Greatest tension is centrally over mons; progressively looser along inguinal crease |
| Direction of pull | In two oblique directions, perpendicular to the lateral limbs of the incision | In one superior-inferior direction, perpendicular to the central incision |
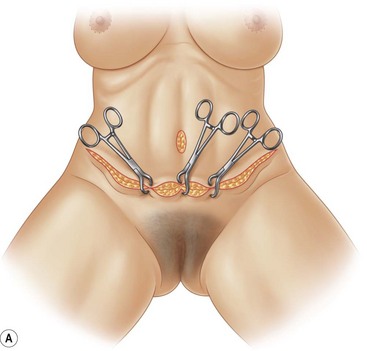
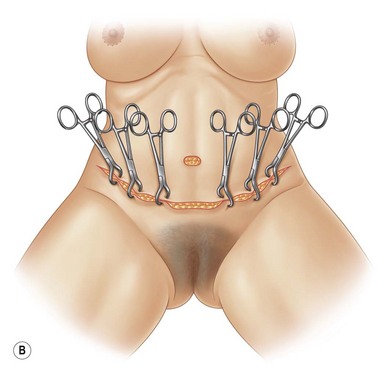
Two years later Lockwood published his HLT paper,2 which was the anterior component of his body lift. He ascribed four key characteristics to the HLT. First, only areas to be excised or necessary for rectus plication would be undermined. Second, simultaneous liposuction would therefore be safe. Third, he used permanent sutures to close the superficial fascial system (SFS) as a means to reduce the widening of scars and to improve skin contour far away from the incision. Finally, he emphasized the importance of putting the greatest tension on the lateral part of the incision.
The higher lateral tension concept also forces us to pay more attention to the scar location. There is a natural tendency to expect the final scar to correspond to the initial incision. But the initial incision has no more to do with the location of the final scar than does the final incision. Both equally determine the amount to be excised, and each needs to be planned carefully (Fig. 25.1).


Preoperative Preparation
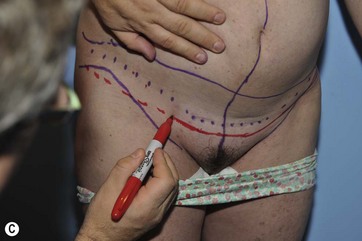
Figure 25.2 shows the preoperative markings. Any abdominoplasty has the potential to correct three separate anatomical structures: skin, fat, and muscle. Each is evaluated separately in order to preoperatively plan the operation and give the patient reasonable expectations.



Skin Excess
One of the signatures of the high lateral tension abdominoplasty is that it requires the greatest tension to be placed on the lateral part of the incision. This means that the umbilical site might not get excised, leaving a vertical scar from its closure. While this usually heals well, and accepting that the presence of this scar may be considered the sine qua non of a true HLT philosophy, this scar does not always heal perfectly, and many patients want to avoid it. If there is any question as to whether the site can be excised, the patient should be warned that there are three choices: proceeding with a classic HLT (Fig. 25.3) and accepting a vertical scar if necessary, placing the incision more superiorly on the abdomen so that there is a greater chance of excising the old umbilical site (though the necessity for elevating the lateral limbs of the flap may make the lateral scar more likely to rise above pants), or abandoning the HLT principles and placing as much central tension as is necessary to remove the site.
Patients frequently ask for a “mini” tummy tuck, wanting the horizontal extent of the incision to be as short as possible, perhaps even as narrow as their C-section scar. Few individuals have vertical laxity so slight and horizontal laxity so centrally focused that a short scar removes all the troubling laxity and attractively recontours the abdomen (Fig. 25.4). The patient should always be evaluated sitting straight upright or even bending forward, as this demonstrates the amount of vertical excess as well as the extent to which the laxity extends laterally. Placing patients in this most unflattering of positions helps them to see the extent of their laxity (Fig. 25.5). They can understand that if there is laxity at the anterior axillary line, then an incision that stops at the midclavicular line will be inadequate to create a nice contour. It can also be demonstrated that if there is a significant amount of vertical excess to be excised, a significant length of the incision is obligatory to avoid a dog-ear. Given that the HLT has greater lateral tension and seeks removal of lateral skin excess, the incision must go even more laterally. Lockwood’s drawings show the superior and inferior incision joined at a 90° angle, but in his discussion he says that the incision needs to be lengthened to eliminate a dog-ear. (This is a reminder that the highest tension is not at the very lateralmost extent of the incision, but is usually located at about the midclavicular line.) An HLT incision will invariably be at least as wide as the anterior axillary line, and often to the posterior axillary line. The philosophy of the standard tummy tuck is to excise the old umbilical site at whatever tension is necessary. The length of the scar is essentially that which is necessary to recontour the abdomen without a dog-ear. But the HLT concept is that the greatest laxity is more lateral, and that it is essential to excise that to optimally tighten the thighs. Placing more tension centrally raises and distorts the mobile mons, oftentimes shortening the distance from the top of the public hair to the umbilicus. Since the mons is more vertically mobile than the skin along the inguinal crease, high central tension causes the mons to rise, making the incision more flat and horizontal, and it is the angle of the lateral limbs that most helps flatten the epigastrium. The HLT concept is that it is better to have a vertical scar from the old umbilical site, with the mons/pubic hair left lower with a greater distance between it and the umbilicus. That is because the standard tummy tuck is essentially an exercise in “excising the umbilicus”; the width is only that which is necessary to remove that vertical excess without creating a dog-ear. But the HLT considers that lateral excess the most important area for excision. By pulling down and out laterally, a greater degree of flattening of the epigastrium occurs than simply pulling straight inferiorly. The greatest laxity on the trunk of the postpartum or weight loss patient is also laterally, so this area needs the greatest amount of excision (Fig. 25.6).
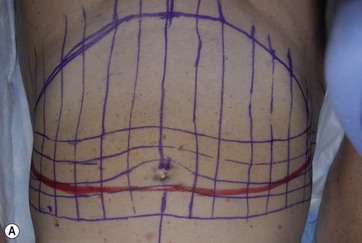
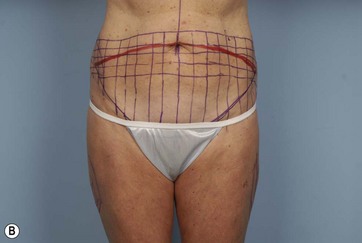
FIG 25.5, 25.6 Appears  ONLINE ONLY
ONLINE ONLY








But the incision often needs to be modified to suit patient expectation. Patients usually want the scar low, horizontal, and the umbilical site excised, despite the fact that it creates a less attractive abdomen. The surgeon is left to negotiate these tradeoffs with the patient. Since many patients do not want a pure HLT, the reader should consider this HLT description as a way of thinking while marking and closing, even if it is not carried out to completion (Table 25.2).
TABLE 25.2 Determination of Final Line of Resection








