Chapter 51 High intensity focused ultrasound and non-invasive body contouring
• High-intensity focused ultrasonic energy (HIFU) is capable of thermal ablation of subcutaneous adipose tissue (SAT) and will modulate collagen found within the midlamellar matrix.
• HIFU does not target vascular structures, unlike laser energy delivered by fiber.
• Following a HIFU treatment, the body removes the cell debris and neocollagenesis occurs over time. The ultimate result of contour improvement is at approximately 12 weeks post-treatment.
• Research studies demonstrate that there are no abnormalities seen in blood chemistry and liver function as the ablated SAT is resorbed.
• The ideal candidate for HIFU body contouring has at least 2.5 cm of tissue on caliper pinch and a BMI <30. HIFU body contouring is not a weight loss treatment, but a way to improve contour where there are areas of fat deposits.
• Ecchymosis in the treatment area is commonly seen, but resolves rapidly afterwards.
• A single treatment with a HIFU device in a research study resulted in at least 2 cm of loss in waist circumference over baseline measurements. There were subgroups of patients that lost an average of 5.68 cm.
• HIFU represents an option for noninvasive body contouring that has an excellent safety profile.
Introduction
Pharmacologic approaches (injection lipolysis or “mesotherapy”) have been considered, yet remain problematic because of the small areas that are treated and the presence of chronic inflammation in tissues.1
Ultrasonic Energy
High intensity, focused ultrasonic energy (HIFU) has been considered as a way to ablate tissue deep inside to body as a treatment for medical conditions (liver metastases, uterine fibroids, and atrial fibrillation.2 Ultrasound propagates through tissue at approximately 1540 m/s. Sonic energy, like light, can be focused. Pressure fluctuations lead to shearing motions and molecular-level interactions that produce heat. Because it is focused to a predetermined point within tissue, the energy can pass across the skin at relatively low fluences of 1–3 J/cm2, yet reach greater than 1000 J/cm2 within the focal zone. In this fashion, a “trackless” lesion is produced, without collateral damage to surrounding tissue or skin. Figure 51.1 demonstrates a Schlieren image of ultrasound waves that converge and diverge beyond a focal zone. Ultrasound can be focused at specific depths within the tissues as demonstrated in Fig. 51.2.
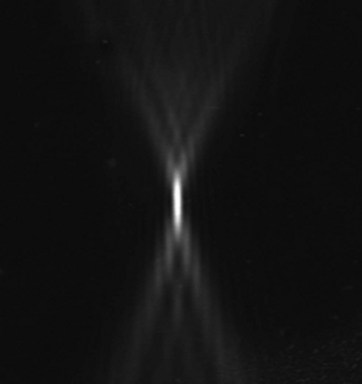
FIG. 51.1 Schlieren photography demonstrates ultrasound converging and diverging around a focal zone.
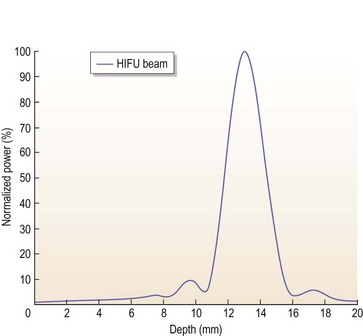
FIG. 51.2 HIFU allows for focused delivery of power at any depth versus other technologies (RF or laser).
Temperature measurements taken within porcine tissue at the focal zone of a commercially available HIFU system (the LipoSonix® system, Medicis Technologies Corporation, Bothell, WA, USA, technical data) approach 70°C, while unaffected nearby tissues are normal (37°C).3
Nonfocused ultrasound is used for bulk heating of tissue by physical therapists in low fluences of 2–5 W/cm2. While this may have a therapeutic benefit for the treatment of musculoskeletal conditions, some devices are capable of bulk tissue heating in the 45–47°C range. This level of tissue heat is problematic in terms of skin burns and tissue necrosis. Currently, a dual-transducer ultrasound device is being studied to determine if it can produce body contour changes. Its use for body contouring would be considered off-label because these devices are approved for tissue heating. The safety and efficacy of external, nonfocused ultrasound as a device for noninvasive body contouring has not been determined. There have been other reports of the use of external, nonfocused ultrasound as an adjunct for the dispersion of wetting solutions used in surgical lipoplasty.4,5 Burns have been reported with nonfocused ultrasound.6
Tissue Thermodynamics
Surgical lipoplasty with ultrasound utilizes a thermal injury protective approach of wetting solutions that prevent excess tissue heating.7 Solid probe devices will fragment tissue at lower energy levels and pulsed energy reduces the possibility of thermal damage.
Tissue Effect and Biology of Thermal HIFU
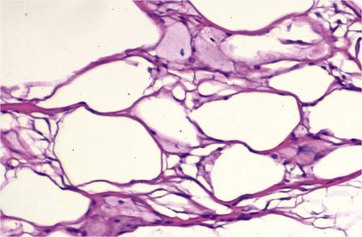
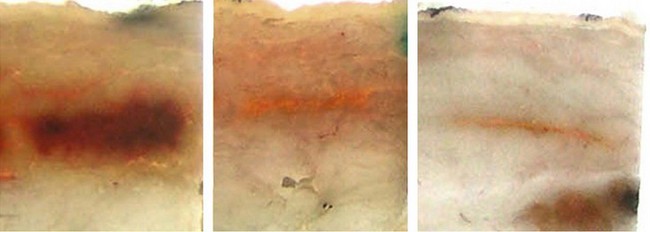
HIFU produces an immediate coagulative necrosis of tissue within its focal zone. A thermal effect is also produced in the collagen component of the MLM. Within the tissue treated with HIFU, a hemorrhagic appearance of the tissue is initially noted, as documented in Fig. 51.3. Extracellular lipid and cell debris is removed by macrophages and transported to the liver via lymphatic channels. Figure 51.4 demonstrates foamy macrophages that are removing cell debris and extracellular lipid. Collagen remodeling occurs over time. The majority of remodeling is completed by week 12, according to animal studies. Within the preclinical and pivotal studies for the LipoSonix device, ecchymosis was frequently seen, yet resolved by 12–16 days post-treatment. Tissue lumpiness or contour irregularities were not encountered. The HIFU lesions within treated tissue heal over time, as shown in Fig. 51.5.

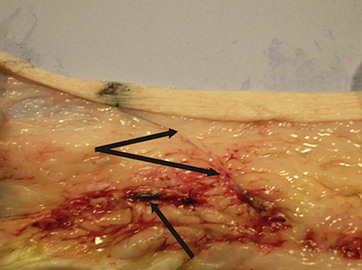
The biologic effect of thermal HIFU appears to be different than other forms of body contouring that use bulk heating of tissue. While adipocyte necrosis results in the release of extracellular lipids, fat necrosis and chronic inflammation following HIFU treatment do not occur. There is minimal collateral damage to tissue, with no known effect on arterioles or lymphatic channels. A patent arteriole that crosses the HIFU treatment zone is seen in Fig. 51.6. Laser frequencies (900–1400 nm) used for lipoplasty (via fiberoptic delivery) are attracted to hemoglobin and water chromophores. This will inflict collateral damage on vascular and lymphatic structures. HIFU, like all other forms of sonic energy, can produce self-limited dysesthesias in cutaneous sensory nerves that are located within the treatment zone.
Thermal HIFU as A Noninvasive Body Contouring Device
Initial studies have established that thermal HIFU has a predictable biologic effect for adipocyte ablation and thermal modulation of collagen contained within the MLM. Safety studies in both preclinical studies, pilot studies and a pivotal study demonstrate that subjects treated with HIFU do not show abnormalities in clinical chemistry laboratory tests that evaluate blood lipids, liver function, inflammatory markers or coagulation during the post-treatment interval.8
The LipoSonix device utilizes a microprocessor-controlled positioning device that moves the transducer head in a water bath to create an X–Y grid pattern that is 5 × 5 cm in dimension, as shown in Fig. 51.7. The transducer head and pattern generating device is seen in Fig. 51.8. Prior to treatment, the areas to be treated are marked with a 5 × 5 cm grid that facilitates placement of the treatment head, as shown in Fig. 51.9. The ultrasonic transducer is energized as it moves through the grid pattern to produce rows of thermal HIFU lesions deep within the treatment zone. Water is the optimal coupling agent between the treatment head and the patient’s skin, as shown in Fig. 51.10. Each treatment zone takes approximately 60 seconds to treat. The energy fluence and depth is adjusted by the operator on the LipoSonix device’s graphic user interface, as seen in Fig. 51.11.
< div class='tao-gold-member'>
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


