Fig. 13.1
(a) HFUS of a nodular BCC (size: 1,844 mm depth × 7,500 mm width; (b) HFUS of a superficial BCC (0,797 mm depth × 12,067 mm width
It seems inconceivable today to examine the skin without the aid of a dermoscope; soon, high-frequency ultrasound (HFUS/HRUS, high-resolution ultrasound, high-resolution echography) should be included in the indispensable armamentarium of those actively working on skin cancer. For some, this has been a common practice for many years [4]. Combining noninvasive techniques (dermoscopy, HFUS, confocal) will save time and money as well as unnecessary biopsies.
The more information is available on a particular tumor, the better treatment can be provided. Clinical evaluation and dermoscopy will give information on the superficial morphologic aspects, HFUS will provide information on shape and volume [5, 6], and confocal microscopy will provide information on cellular aspects [7] (Fig. 13.2a–d).
Fig. 13.2
(a–d) Four ways of looking at a nodular BCC: (a) clinical photograph, (b) dermoscopic image, (c) HFUS, (d) confocal microcopy (d: Courtesy of Rainer Hofmann-Wellenhof, MD)
There is an excellent correlation between dermoscopy and HFUS dimensions [5]. This means that the dimensions obtained by dermoscopy correspond to the HFUS length of the tumor. Therefore, the dermoscopy image corresponds to the real size of the tumor; however, only through HFUS one will know the actual depth and shape of the tumor.
Some tumor characteristics that can be better understood by HFUS evaluation are:
Volume/Shape. The shape and size of a tumor can provide information of the type of tumor. Most BCC are anechoic and have a roughly elliptical shape; occasionally, they are elongated anechoic and have a collar necklace or rosary pattern (Fig. 13.3). SCC are also hypoechoic, but a thick superficial crust needs to be removed before visualization [4]. They are usually thick lesions with irregular “iceberg” shapes. HFUS imaging will be of great help in choosing the proper site for biopsy or selecting the best method for tumor removal. In addition, some tumors have an iceberg shape: they appear small at the surface while the length underneath the surface is larger. This could be the cause of positive margins after surgery.
Fig. 13.3
Collar necklace HFUS image of a superficial BCC
Depth. The knowledge of the depth of tumors helps in deciding the correct surgical technique. For example, superficial BCC lesions can be diagnosed by clinical/dermoscopy [8] examination. Treatment options include cryosurgery, topical immunomodulators like imiquimod, photodynamic therapy (PDT), and curettage/electrocoagulation, among others. There is no need for costly, lengthy, expensive, and invasive techniques like Mohs micrographic surgery on a superficial carcinoma. Although this seems logical, the out-of-proportion use of Mohs surgery (1 out of every 4 tumors are treated with MMS [9]) suggests that this technique is being used for treating many superficial lesions. The HFUS image of a superficial BCC shows a hypoechoic elliptical area(s) of less than 1 mm of depth. Individually, each island of tumor measures 1–1.2 mm in depth. Lengthwise, they can be small (1–2 mm) but can also be quite large, requiring a segmental HFUS evaluation in order to cover the whole area. HFUS allows the determination as to whether BCC is only superficial or it has a deeper component within the tumor. Apparently “superficial BCC” can “hide” nodular or even morpheaform elements (admixture tumor), as is the case in roughly one-third of all BCC [10, 11] (Fig. 13.4a, b). The latter is a common cause of treatment failure and recurrence (Fig. 13.5). Sometimes this reoccurrence is many years later. The tumor’s depth has to be determined throughout the whole tumor area using HFUS readings. The deep margin evaluation by HFUS is limited to tumors under 8 mm in depth. Proper selection of the biopsy site is of utmost importance [12]; therefore, HFUS-guided biopsy could be another possible indication.

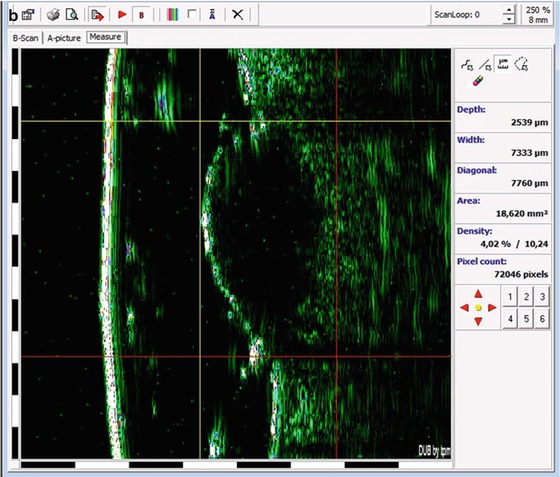
Fig. 13.4
(a, b) A very large pigmented BCC on the back. (a) Clinical evaluation and dermoscopy showed a superficial BCC with an ulcerated area (circle). (b) HFUS showed a nodular area
Fig. 13.5
Same patient as in Fig. 13.4. BCC was treated with topical imiquimod treatment. After healing from the imiquimod treatment, there was residual tumor (corresponding to the nodular part). This residual tumor was later treated with cryosurgery (close technique)
Length. The longitudinal/width margin evaluation by HFUS is limited to tumors under 12 mm. For large lesions, HFUS might need to be performed by sectors.
13.2 HFUS and Cryosurgery
The combination of HFUS and cryosurgery has the following advantages:
1.
This combination gives the surgeon information regarding the volume, depth, and length of the tumor.
2.
This combination allows for visualization of the depth of the freezing front.
13.3 HFUS Volume and Cryosurgery
Cancer cells need a temperature of at least – 50 ºC to be destroyed. That temperature must be reached throughout the entire tumor including the safety margin of 4 mm. The temperature at the center of the freezing ball is the first to achieve the optimal killing temperatures. The concern is at the periphery of the tumor where suboptimal freezing temperatures might leave undestroyed malignant cells. Therefore, temperature needs to be measured at the periphery. Following the isotherm, the temperature at the depth of the tumor can be inferred (Fig. 13.6).
Fig. 13.6
The ice ball expands in a roughly hemispherical shape. The temperature decreases from the center out in isotherm. The lateral spread from the edge of a probe is approximately equal to the depth of the freeze. The temperatures at the base and at the lateral margin are the same
Deep tumors are best treated with close (probe) or chamber technique because a greater depth is reached (Fig. 13.7). In general, the length/depth ratio is 6 × 1 (for nodular BCC the ratio is 4 × 1) [5]. Superficial/shallow tumors can be treated both by open (spray) or close (probe) technique.
Fig. 13.7




The volume ratio of most nodular BCC measured by HFUS is 4 × 1. The ice ball of a close (probe) cryosurgery is approximately 4 × 2; for spray, cryosurgery has a hat shape, and it is approximately 4 × 1.5 (these last two shapes were obtained from a gelatin model)
Related posts:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
