Herpes Zoster and Varicella
Jeffrey M. Melancon
I. BACKGROUND
Infection with the varicella-zoster virus (VZV), a double-stranded deoxyribonucleic acid (DNA) virus, will produce one of two clinical entities. Generalized, highly contagious, and usually benign chickenpox represents primary infection in a nonimmune host, whereas localized and painful zoster, more commonly known as shingles, is recurrence of a latent infection in the partially immune host. Clinical manifestations reflect the interaction between the VZV and the host immune mechanisms.
Varicella infection, commonly known as chickenpox, is usually acquired through respiratory droplets. The disease is seen primarily in the winter and spring, has an incubation period of 10 to 23 days, begins abruptly, and lesions heal or even disappear within 7 to 10 days. Ninety percent of reported cases occur in children <10 years of age. Four percent of infections are subclinical. Almost every individual would have been infected by young adulthood. The disease is communicable from 1 day before the appearance of the exanthem to 6 days after; crusts are noninfectious. Signs, symptoms, and complications often become more severe with age; adolescents and adults may become severely ill, particularly with pulmonary involvement.
Primary VZV infections during pregnancy, although rare, can cause serious problems for both the mother and the child. The implications of primary infection vary significantly with the gestational age at infection. For the mother, the risk of severe illness is greatest after mid-pregnancy, when she is relatively immunocompromised. For the fetus, the risk of congenital infection is greatest when maternal infection occurs in the first or second trimester. Maternal infection is preventable by preconception vaccination.1 Varicella pneumonia complicates up to 20% of cases of VZV infections in pregnancy. Symptoms usually appear about 4 days after the onset of the rash and may include cough, shortness of breath, chest pain, and hemoptysis. Congenital varicella syndrome, characterized by limb hypoplasia, muscular atrophy, skin scarring, cortical atrophy, microcephaly, cataract formation, and rudimentary digits, may also result from maternal varicella infection. The risks of these comorbid conditions are calculated to be 0.4% or 2% if infection occurs in the first 12 to 20 weeks.2
Zoster results from the reactivation of latent virus in dorsal root or cranial nerve ganglion cells. It is suspected that the virus is transported from the dorsal root or trigeminal ganglia through the myelinated nerves to the skin. As these nerves may terminate at the isthmus of hair follicles, primary infection first occurs in the follicular and sebaceous epithelium and then spreads to the rest of the epidermis. Histologic evidence reveals that zoster infection may occur exclusively in the folliculosebaceous units before the clinical appearance of vesicles.3
The incidence of zoster shows no seasonal variation. Two-thirds of patients are older than 40 years. Lesions erupt for several days and are usually
gone within 2 to 3 weeks in children and 2 to 4 weeks in adults. Zoster is a self-limited, localized disease that causes discomfort for several days but usually heals without complications. Postherpetic neuralgia (PHN) is seen with increasing frequency in those older than 60 years of age and can be extremely painful and sometimes chronic.
gone within 2 to 3 weeks in children and 2 to 4 weeks in adults. Zoster is a self-limited, localized disease that causes discomfort for several days but usually heals without complications. Postherpetic neuralgia (PHN) is seen with increasing frequency in those older than 60 years of age and can be extremely painful and sometimes chronic.
In patients with serious underlying conditions that alter immunologic competence, more severe disease develops. Lesions may be greater in number and persist for up to 7 months in the immunosuppressed; visceral dissemination can occur in 8% of untreated immunocompromised patients. For children with lymphoma or leukemia, varicella is a life-threatening infection; adults with such diseases often develop zoster, which may then disseminate. Dissemination occurs in only 2% to 4% of zoster cases in normal hosts. However, approximately two-thirds of patients with disseminated zoster have malignant disease. In patients known to be at risk for acquired immunodeficiency syndrome (AIDS), the occurrence of zoster may be one sign that heralds depression of cellular immunity and may be the first sign of human immunodeficiency virus (HIV) infection. HIV-infected patients may experience more severe primary infection or atypical varicella occurring concurrently with zoster.4
II. CLINICAL PRESENTATION
A. Varicella. Varicella in children is preceded by little or no prodrome; there may be only 24 hours of malaise and fever. In adolescents and adults, fever and constitutional symptoms almost always precede the exanthem by 24 to 48 hours. Patients are usually infectious for 1 to 2 days before the development of the rash and for 4 to 5 days following the beginning of the eruption, which is usually when the last vesicular crop has crusted. Patients often experience intense pruritus with the vesicular stage. The appearance of cough, dyspnea, and chest pain within 2 to 5 days after the onset of the rash is indicative of severe pulmonary involvement. Pruritus is the primary and most troublesome feature of chickenpox. Excoriation contributes to secondary bacterial infection and scarring.
Chickenpox begins abruptly with the appearance of discrete, erythematous macules and papules located primarily over the thorax, scalp, and mucous membranes; the face and distal extremities remain less involved (Fig. 19-1). Lesions progress rapidly from erythematous macules to 2 to 3 mm clear, tense, fragile vesicles surrounded by an erythematous areola. This appearance is often descriptively coined as “dew drops on a rose petal.” As the lesions progress, they first become umbilicated and then within hours become cloudy and purulent, with crusts forming in 2 to 4 days. Varicella lesions appear in 3 to 5 distinct crops for up to a 5-day period, and lesions in all stages of development may be seen within one area (Fig. 19-2). This is an important difference from smallpox. Crusts fall off in 1 to 3 weeks. Lesions usually heal without scarring. The most common complications are secondary bacterial infection of the skin lesions, usually staphylococci and streptococci. Adults often have a more complicated course with a more widespread rash, a prolonged fever, and an increased chance of complications, most commonly varicella pneumonia.
B. Herpes Zoster. The appearance of zoster lesions is frequently preceded by a mild-to-severe pre-eruptive pruritus, tenderness, or pain. The pain may be generalized over the entire nerve segment, localized to part of it, or referred.
Depending on the location, this pain may be confused with that of pleural or cardiac disease, cholecystitis or other abdominal catastrophe, renal or ureteral colic, sciatica, or other ailments. Neurologic changes within the affected dermatome include hyperesthesia, dysesthesia, and hypoesthesia. The interval between pain and eruption may be as long as 10 days but averages 3 to 5 days. In some patients, particularly children, there are no sensory changes. The pain will usually subside within several weeks, but 73% of patients older than 60 years of age have discomfort that persists beyond 8 weeks.
Depending on the location, this pain may be confused with that of pleural or cardiac disease, cholecystitis or other abdominal catastrophe, renal or ureteral colic, sciatica, or other ailments. Neurologic changes within the affected dermatome include hyperesthesia, dysesthesia, and hypoesthesia. The interval between pain and eruption may be as long as 10 days but averages 3 to 5 days. In some patients, particularly children, there are no sensory changes. The pain will usually subside within several weeks, but 73% of patients older than 60 years of age have discomfort that persists beyond 8 weeks.
 Figure 19-1. Varicella. (From Centers for Disease Control and Prevention Public Health Image Library.) |
 Figure 19-2. Varicella. Note the various stages of the lesions: papular, vesicular, and crusted lesions. (Courtesy of Shirley P. Klein, MD.) |
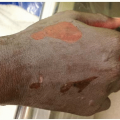
Zoster lesions first appear posteriorly and progress to the anterior and peripheral distribution of the nerve involved (see dermatome charts on the inside covers). Only rarely will the eruption be bilateral. Erythematous macules, papules, and plaques are seen first, and in most instances grouped vesicles appear within 24 hours, although occasionally blisters never develop. Plaques may be scattered irregularly along a dermatomal segment or may become confluent (Fig. 19-3). Mucous membranes within the dermatomes are also affected. The vesicles become purulent, crust, and fall off within 1 to 2 weeks. The presence of a few vesicles (10 to 25) outside the affected dermatome can occur and does not imply dissemination.
In >50% of individuals, zoster will involve the thoracic nerves; cervical or lumbar nerve involvement occurs in 15% to 20% of cases. Lesions on the tip of the nose herald involvement of the nasociliary branch of the ophthalmic division of the trigeminal nerve, implying a strong possibility of concomitant keratoconjunctivitis. Referral to an ophthalmologist for evaluation of ocular involvement is recommended. When herpes zoster occurs along the facial nerve and involves the geniculate ganglion—it may be accompanied by symptoms such as hearing loss and a rapid onset of facial pain. This combination of symptoms may indicate herpes zoster oticus, also called Ramsay Hunt syndrome (Fig. 19-4). On physical examination, there may be a unilateral herpetic rash of the pinna and peripheral facial paralysis. Patients may also experience a loss of taste and vertigo. Paresis and permanent motor damage are more common than previously thought and are found mostly with involvement of the trigeminal and upper cervical and thoracic nerves. Shingles may appear in multiple
dermatomes both contiguous and noncontiguous and this is termed zoster multiplex,5 which is more common in immunocompromised individuals. VZV may reactivate without causing cutaneous vesicles but instead present with other symptoms and is termed zoster sine herpete. Overall incidence is 10% to 20%, with >66% of individuals affected with zoster being older than 50 years of age. Twenty-five percent of patients with HIV and 7% to 9% of patients with renal and cardiac transplant experience at least one episode of zoster. Ninety-five percent to 100% of individuals are seropositive for VZV antibodies. The disseminated form of zoster occurs in 2% to 20% of patients with herpes zoster, while up to 35% of patients with localized zoster will have a few scattered vesicles in remote sites. Those patients predisposed to more severe disease may show hemorrhagic, bullous, and infarctive-gangrenous lesions, which will heal slowly with scarring. Persistent varicella zoster in an immunocompromised host may present with atypical hyperkeratotic papules.
dermatomes both contiguous and noncontiguous and this is termed zoster multiplex,5 which is more common in immunocompromised individuals. VZV may reactivate without causing cutaneous vesicles but instead present with other symptoms and is termed zoster sine herpete. Overall incidence is 10% to 20%, with >66% of individuals affected with zoster being older than 50 years of age. Twenty-five percent of patients with HIV and 7% to 9% of patients with renal and cardiac transplant experience at least one episode of zoster. Ninety-five percent to 100% of individuals are seropositive for VZV antibodies. The disseminated form of zoster occurs in 2% to 20% of patients with herpes zoster, while up to 35% of patients with localized zoster will have a few scattered vesicles in remote sites. Those patients predisposed to more severe disease may show hemorrhagic, bullous, and infarctive-gangrenous lesions, which will heal slowly with scarring. Persistent varicella zoster in an immunocompromised host may present with atypical hyperkeratotic papules.
 Figure 19-3. Herpes zoster. (From Goodheart HP. Goodheart’s Photoguide of Common Skin Disorders. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2003.) |
 Figure 19-4. Herpes zoster-Ramsey Hunt syndrome. |
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


