Herpes Simplex
Jeffrey M. Melancon
I. BACKGROUND
Cutaneous herpes simplex infections take two distinct forms: (i) the painful and disabling primary infection of previously uninfected individuals and (ii) the common, bothersome, recurrent form colloquially known as cold sores or fever blisters. These infections are asymptomatic in up to 80% of patients. The mode of transmission is by close personal contact. The virus is inoculated either through mucous membranes or through small cracks in the skin. By 4 years of age, approximately 50% of the population has antibodies to herpes simplex virus (HSV), indicative of prior exposure. This percentage increases to 60% to 70% by age 14. Following primary infection, effective immunity develops in some individuals, but 20% to 45% will have recurrent disease, and 7% of the general population has at least two episodes of recurrent orolabial HSV per year.
Herpes simplex is a DNA virus infecting humans alone that has an almost universal distribution. There are two types of HSV: type 1, which is usually responsible for nongenital herpetic infections; and type 2, which is usually the agent involved in genital infections in both men and women. It is important to recognize that the herpes virus has three unique properties. It has the capacity to invade and replicate within the nervous tissue. The virus then remains latent within the neural tissue, most commonly the trigeminal ganglia for HSV-1 and the sacral ganglia for HSV-2. Lastly, the latent virus has the capacity to reactivate and replicate causing cutaneous disease. There are certain biologic differences between the two types. For example, HSV-2 genital infections recur more frequently than HSV-1 genital herpes. However, nongenital HSV-1 infections recur more frequently than nongenital herpes due to HSV-2. Genital HSV infections recur sixfold more frequently than orolabial HSV infections. Previous infection with one type of HSV does not appear to provide effective immunity to subsequent infection with the other.
True primary infection occurs in a person with no previous exposure to HSV and is usually quite severe. First-episode genital infections can occur in persons who either had previous nongenital HSV infection or have serologic evidence of prior subclinical exposure to the virus. Although not sufficient to prevent reinfection, this degree of immunity at least confers partial protection such that first-episode genital infection is less severe than a true primary one. The primary infection has an incubation period of 3 to 12 days following exposure and runs a clinical course of 1 to 3 weeks. Viral excretion persists for 15 to 42 days after the primary infection. Recurrent lesions heal more quickly (7 to 10 days), and in recurrent orofacial disease most lesions are no longer excreting virus by 5 days. In women with recurrent genital herpes, virus is present for a mean of 4.8 days, while 16% may continue to shed virus from lesions
after 6 days. Asymptomatic shedding of HSV has also been demonstrated from both oropharyngeal and genital sites at low rates without evident lesions. The most recent studies suggest that transmission of genital herpes occurs most frequently from persons who asymptomatically shed virus. The annual risk of transmission from a sexual partner with genital herpes in a heterosexual relationship is approximately 10%.
after 6 days. Asymptomatic shedding of HSV has also been demonstrated from both oropharyngeal and genital sites at low rates without evident lesions. The most recent studies suggest that transmission of genital herpes occurs most frequently from persons who asymptomatically shed virus. The annual risk of transmission from a sexual partner with genital herpes in a heterosexual relationship is approximately 10%.
Genital herpes simplex is one of the most common sexually transmitted diseases (STDs). The prevalence of HSV-2 infection in the United States has been estimated to range from 20% to 60%. Even without considering its significant psychosocial impact, genital herpes simplex infection may pose other health problems for female patients. Pregnant women with a history of genital herpes must be carefully monitored. Women who have active, recurrent genital herpes should be offered suppressive viral therapy at or beyond 36 weeks of gestation, whereas Cesarean delivery is indicated in women with active genital lesions or prodromal symptoms (e.g., vulvar pain and burning) at the time of delivery.1 The risk of HSV infection in neonates exposed to the virus at the time of vaginal delivery to mothers with a history of recurrent genital HSV infections is very low (≤8%). The presence and titer of neutralizing antibody to HSV contribute to this low rate. In contrast, infants born to women with a primary HSV infection have a more than 50% risk of developing a clinical infection; Cesarean delivery is indicated. Neonatal herpes simplex infection is a serious disease with up to a 50% mortality rate and a significant chance of permanent sequelae among its survivors. Up to 60% to 80% of babies infected with HSV are delivered by women with no evidence of clinical HSV on examination. Disease during early pregnancy may produce malformations that are clinically indistinguishable from those produced by cytomegalovirus. Anorectal herpes is being recognized with increased frequency. When caused by HSV-2, it is usually transmitted by anal intercourse. HSV-1 causes perianal infections in immunosuppressed patients, presumably by autoinoculation from orofacial lesions.
After primary infection, the virus appears to remain latent in sensory ganglia. In patients with recurrent herpes, the virus is periodically reactivated and conducted to the epidermis through peripheral nerve fibers. It then replicates in the skin, producing the recurrent herpetic lesion. Trigger factors include emotional stress, physical trauma (including genital trauma), sunburn, menses, fever, and systemic infections. The long-term natural history of recurrent nongenital herpes infection is not well characterized. The virus type influences the recurrence rate of genital herpes, as does gender, with men being at greater risk for recurrent disease. There is a great deal of variation in recurrence rates among individuals. Over time, most patients experience clinically significant reductions in disease severity. Rates of recurrence begin to decline by the second year after initial outbreaks.2
Patients with atopic dermatitis risk the development of generalized lesions (eczema herpeticum), regardless of whether their eczema is active. Diseases or drugs that interfere with host response, particularly with cell-mediated immunity, also predispose to widespread, slowly healing, and more destructive infections. Those patients with lymphoreticular malignancies or thymic defects and immunosuppressed transplant or acquired immunodeficiency syndrome (AIDS) are most prone to severe HSV infections.
II. CLINICAL PRESENTATION
A. Primary Symptomatic Oral or Genital Herpes Simplex Virus Infections. Infections on mucosal surfaces are preceded by a day or two of local tenderness. The lesions are accompanied by severe pain and tender lymphadenopathy, often making it impossible for those with gingivostomatitis to eat or drink or patients with extensive genital involvement to walk or urinate. High fever and purulent malodorous secretions accompany oral and vaginal infections. Primary genital infection in men usually results in painful penile lesions. It may also cause urethritis with dysuria and discharge. Anorectal infection may be complicated by tenesmus, constipation, and urinary retention.
Acute herpetic gingivostomatitis is the most frequent manifestation of primary infection, usually seen in young children. It is usually abrupt at onset and is associated with a high fever, anorexia, and listlessness. This acute episode lasts from 5 days to 1 week. Vesicles, erosions, and maceration are seen over the entire buccal mucosa; this can involve the perioral skin because of contamination. Marked erythema and edema of the gingiva are typical. Submandibular adenopathy is usually present and is tender. Acute herpetic pharyngotonsillitis is usually seen in adults and is an oropharyngeal infection of HSV-1. Symptoms are usually a sore throat, fever, malaise, and headache. HSV-2 can be an etiologic agent; however, this usually involves orogenital contact.
Vulvovaginitis is seen most frequently in girls and young women. It consists of widespread vesicles, erosions, and edema in the vulva, labia, and surrounding skin. These areas become very edematous, erythematous, and extremely tender. A profuse vaginal discharge is present, and some women develop urinary retention. Bilateral tender inguinal adenopathy is usually present. Cervicitis is often asymptomatic but nevertheless important to recognize in pregnant women because of the associated risk of fetal infection and spontaneous abortion. Pregnant women who acquire genital herpes during the first 20 weeks of pregnancy have an increased risk of abortions, whereas the infants of those who acquire an infection after 20 weeks have an increased incidence of prematurity and birth defects. Urethritis in men is accompanied by a watery discharge and the occasional presence of vesicles around the urethral meatus. Anorectal herpes is characterized by the typical cutaneous lesions as well as rectal ulcerations. Extensive indolent lesions are not uncommon in patients with AIDS. In the United States, genital ulcers are most commonly caused by HSV-2. These ulcers may contain multiple pathogens, and the patient should be evaluated for coexisting STDs. Most of the episodes of primary genital herpes are asymptomatic and up to 80% have no history of symptomatic genital herpes.
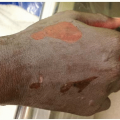
Inoculation herpes is commonly found on the paronychial area (herpetic whitlow) (Fig. 18-1) of nurses and physicians, particularly those involved with mouth care, and may also be found on previously traumatized or burned skin. The lesions are characterized by the sudden appearance of vesicles and are accompanied by extreme local pain, sometimes a sterile lymphangitis, and rarely a systemic reaction. The first episode may last up to 28 days. Recurrent infections most often occur in adults with HSV-2 infection. Herpetic whitlow is often misdiagnosed as a bacterial paronychia and mistreated with incision and drainage of lesions, with subsequent implantation of the virus into the
incised tissue. Herpes gladiatorum occurs among wrestlers, secondary to contact with opponents with active herpes virus infection.
incised tissue. Herpes gladiatorum occurs among wrestlers, secondary to contact with opponents with active herpes virus infection.
 Figure 18-1. Herpetic whitlow. (From Berg D, Worzala K. Atlas of Adult Physical Diagnosis. Philadelphia, PA: Lippincott Williams & Wilkins; 2006.) |
B. Recurrent Herpes Simplex Virus Infections.




Related posts:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
