Hands and Fingers
OVERVIEW
The hands and fingers are the workhorses of the body, constantly in contact with, and exposed regularly to the external environment in all seasons. Sun exposure, soaps, and other harsh contactants are daily insults and irritants. Fortunately, the palmar surfaces are adapted with a thick stratum corneum that is a much more resilient barrier than the stratum corneum on the dorsal surfaces; thus, the palms experience less frequent episodes of irritant and allergic contact dermatitis. In contrast, the dorsal surfaces are much more likely to develop both irritant and allergic contact dermatitis as well as sun-induced atypical lesions.
The fingers and periungual areas can offer hints to diagnosing autoimmune disorders such as systemic lupus erythematosus, dermatomyositis, and scleroderma.
HANDS, FINGERS, AND TOES OF YOUNG CHILDREN
Scarlet fever (SF), toxic shock syndrome (TSS), and Kawasaki disease (KD) all exhibit palmoplantar desquamation. SF and TSS are most commonly triggered by an erythrogenic exotoxin-producing strain of group A beta-hemolytic streptococci or staphylococcal species. The cause of KD is unknown.
Scarlet Fever
The palmar and plantar desquamation of scarlet fever (SF) may follow a streptococcal pharyngitis or tonsillitis. SF typically begins with the abrupt onset of fever, sore throat, and a finely papular exanthem, with a distinctive “sandpapery” or “scarlatiniform” texture.
Distinguishing Features
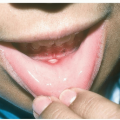
During the convalescent phase of the illness, the skin of the palms and soles frequently desquamates. The desquamation may be sheet-like (Fig. 14-1, A and B).
Toxic Shock Syndrome
Toxic shock syndrome (TSS) is a systemic illness caused by infection with toxin-producing strains of Staphylococcus aureus or, less often, streptococci. Originally described in association with tampon use in women, TSS now occurs more commonly secondary to a local wound infection. Streptococcus and Staphylococcus can produce circulating toxins that cause clinical disease. Many of these toxins function as superantigens with resultant excessive production of pro-inflammatory cytokines and T cell proliferation, causing clinical symptoms that include fever, hypotension, and shock.
Distinguishing Features
Symptoms include erythema and edema of the palms and soles, as well as desquamation that occurs 1 to 3 weeks after the onset of illness (Fig. 14-2)
Kawasaki Disease
Kawasaki disease (KD), also known as mucocutaneous lymph node syndrome, is most often seen in those with Japanese ancestry. KD is a multisystem vasculitis that primarily affects infants and children. Evidence suggests an inhaled antigen triggers an immune response in genetically susceptible hosts. Symptoms include desquamation of the fingers and toes. (A similar multisystem inflammatory condition has been associated with COVID-19, especially in children [see Cutaneous Manifestations of COVID-19].)
 Figure 14-1 A and B. Streptococcal scarlet fever, desquamation. Skin peeling from this boy’s soles (A) and palms (B) during the convalescent phase of his illness. This exuberant desquamation occurred 2 weeks after he had fever and a truncal exanthem that began as a streptococcal throat infection. |
 Figure 14-2 Toxic Shock Syndrome. Desquamation of the feet and toes after toxic shock. (Reprinted with permission from Lugo-Somolinos A, McKinley-Grant L, Goldsmith L, et al. Visual Dx: Essential Dermatology in Pigmented Skin. Wolters Kluwer; 2011.) |
 Figure 14-3 Kawasaki Disease (Mucocutaneous lymph node syndrome). Edema of the hand in this child. |
Distinguishing Features
Erythema of palms and soles, indurative edema of the hands (Fig. 14-3) and feet, followed by desquamation of the fingertips
DORSAL SURFACE OF HANDS
Granuloma Annulare
Granuloma annulare (GA) is an idiopathic, generally asymptomatic, ring-shaped grouping of dermal papules. Proposed pathogenic mechanisms include cell-mediated immunity (type IV), immune complex vasculitis, and an abnormality of tissue monocytes. The papules are composed of focal granulomas that coalesce to form curious circles or semicircular plaques which can be easily misdiagnosed as “ringworm.” Rare cases persist for decades or longer.
GA is seen most frequently in young children in whom it is most often self-limiting. It also appears in adult women (female-to-male ratio is 2.5:1), in whom GA tends to be more chronic. There is an adult form of disseminated GA, which may be associated with diabetes.
Distinguishing Features
Lesions are red, pink, or skin-colored firm dermal papules that most often arise on the dorsal surfaces of the hands, fingers, and feet (see Fig. 19-14), less often, on the extensor aspects of the arms and legs

Figure 14-4 Granuloma annulare.
Erythematous annular and arcuate (crescent-shaped), dermal papules.
May be individual, isolated papules or joined in annular or semiannular (arciform) plaques with central clearing (Fig. 14-4)
Lesions have no epidermal change (i.e., scale)
Centers of lesions may be slightly hyperpigmented and depressed relative to their borders
Generally asymptomatic; primarily a cosmetic concern
In adults, GA may also be found on the elbows, trunk, legs, and neck
Subcutaneous nodules similar to rheumatoid nodules may be seen on arms and legs
In the generalized form, multiple small, skin-colored, erythematous or violaceous lesions appear on the trunk and, to a lesser extent, on the limbs. The distinctive annular pattern is not always present
Diagnosis
Most often made on clinical grounds
Skin biopsy, if the diagnosis is in doubt. GA has a characteristic histopathology consisting of foci of altered collagen and mucin surrounded by granulomatous inflammation of histiocytic and lymphocytic cells. The degenerative collagen is referred to histopathologically as necrobiosis
Management
Localized lesions in very young children are often best left untreated
Potent topical steroids, if desired, may be used alone or under polyethylene occlusion with corticosteroid-impregnated tape (Cordran Tape)
Intralesional triamcinolone acetonide (Kenalog) in a dosage of 2 to 5 mg/mL is injected directly into the elevated border of the lesions with a 30-gauge needle
Phytophotodermatitis
Phytophotodermatitis, also known as berloque dermatitis, is a phototoxic reaction that results from contact with a photosensitizing agent followed by sun exposure. It is a phototoxic reaction from contact with certain plants. Its name has three components: phyto (plant), photo (light), and dermatitis (inflammatory eczematous rash).
The photosensitizing chemicals called furocoumarins are commonly found in several citrus fruits and plants, including lemons, limes, bergamot oranges, grapefruit, celery, parsley, parsnip, and hogweed.
The reaction is a chemically induced, nonimmunologic, acute skin reaction requiring sunlight. A botanical cause for dermatitis is suspected when the pattern of an eruption is linear or streaky, such as noted in the contact dermatitis caused by poison ivy. When the phytophotodermatitis is caused by perfume or other agents such as oil from the bergamot orange, an ingredient formerly contained in certain perfumes and fragrances, it is referred to as berloque dermatitis.
Distinguishing Features
Occurs during the spring or summer following an outdoor activity, such as squeezing lemons or limes on chicken or fish while outdoor barbequing, or from contact with one of the responsible plants
The initial skin response resembles an exaggerated sunburn which may be accompanied by blisters (Fig. 14-5, A). The reaction typically begins within 24 hours of exposure and peaks at 48 to 72 hours
Postinflammatory hyperpigmentation that may last several weeks or longer typically ensues (Fig. 14-5, B)
Management
Reassurance, since lesions fade over the course of a few weeks; no treatment is necessary
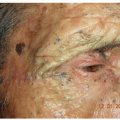
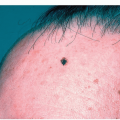
Solar Lentigines vs Seborrheic Keratoses
Solar lentigines, or “liver spots,” that appear on the sun-exposed dorsal hands, are often indistinguishable from seborrheic keratoses that also appear in this location. Solar lentigines are small, tan, oval to geometric shaped macules that are uniformly pigmented (Fig. 14-6). Seborrheic keratoses are flat or slightly palpable and may have a scaly or warty surface (Fig. 14-7).
 Figure 14-5 A and B. Phytophotodermatitis. A, This woman was squeezing limes for an outdoor barbecue 2 days before this blistering eruption began. B, This is the same patient 2 weeks later. Note the postinflammatory hyperpigmentation that faded shortly thereafter. |
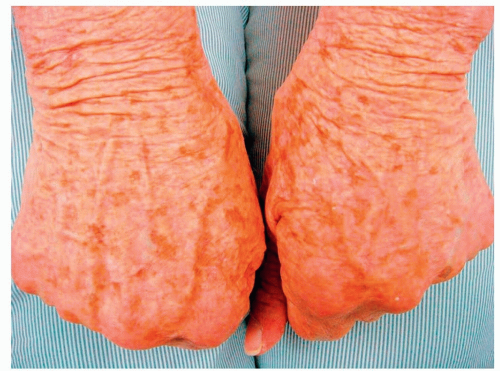 Figure 14-6 Solar Lentigines. Small uniformly pigmented macules. |
 Figure 14-7 Seborrheic keratoses. Small whitish-tan scaly, warty papules. |
 Figure 14-8 Actinic keratoses. Multiple elevated rough-textured papules with white scale overlying sun damaged skin. |
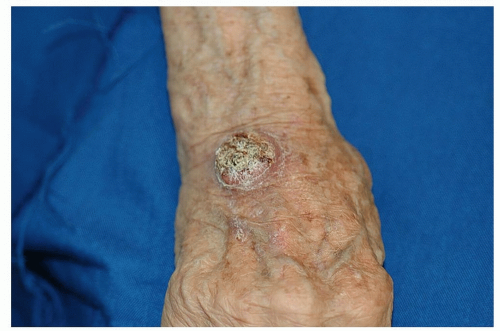 Figure 14-9 Squamous cell carcinoma. A well-differentiated SCC with a thick hyperkeratotic surface. |
PALMAR SURFACE OF HANDS
Hand Eczema
Hand eczema is a very common condition that is seen most often in those who have an underlying atopic predisposition. For descriptive purposes, Hand and foot eczema may be divided into two clinical presentations: a “wet” dyshidrotic type and a “dry,” hyperkeratotic, scaly type. The term dyshidrotic is a misnomer based on the erroneous assumption that the eczematous vesicles are caused by trapped sweat. We now understand that the vesicles result from inflammation and foci of intercellular edema (spongiosis), which becomes loculated in the thick stratum corneum.
Both endogenous hand eczema, where there is a personal or family history of atopy, and exogenous hand eczema, where irritants, allergens, or microbes are contributory factors, are often at work in the same patient.
Irritant contact dermatitis (ICD) and allergic contact dermatitis (ACD) are frequent occupational hazards. ACD is a delayed type IV hypersensitivity reaction that typically occurs days after exposure to a contactant such as solvents, oils, cement, metal (nickel), rings, topical medications, rubber gloves in surgeons, cosmetics, and countless other agents. Both ICD and ACD are also common concerns for those who work in industries that involve cleaning, hairdressing, painting, and metalwork. Eczema due to an irritant or allergen is less commonly seen on the palmar and plantar surfaces due to their much thicker stratum corneum than is found on the dorsal hands and feet.
Dyshidrotic Eczema Distinguishing Features
Dyshidrotic eczema, the “wet” vesicular type, or pompholyx (the Greek word for bubble), is characterized by the following:
Intensely itchy, clear vesicles that are typically located on the palms and sides of the fingers; can also occur on the soles of the feet and the lateral aspects of the toes
Initially, the vesicles are very small and clear and resemble little bubbles (Figs. 14-10 and 14-11)
Later, as they dry and resolve without rupturing, they turn into golden brown vesicles and pustules (Fig. 14-12) that are most often sterile; however, secondary bacterial infection (impetiginization) may occur
 Figure 14-10 Dyshidrotic eczema, pompholyx. These are itchy, clear vesicles (“wet type” hand eczema) that are typically located on the palms and sides of the fingers. |
 Figure 14-11 Dyshidrotic hand eczema, pompholyx. Vesicles on the sides of the fingers and webspace are shown here. |
 Figure 14-12 Dyshidrotic hand eczema, pustular. Itchy, erythematous, vesicles, crusts, and pustules. (Image courtesy of Mark Lebwohl, MD.) |
Hyperkeratotic Hand Eczema Distinguishing Features
Hyperkeratotic, the “dry,” scaly type of hand eczema, is characterized by the following:
Scaly, itchy, erythematous plaques; skin surface loses flexibility and often develops painful fissures (Fig. 14-13)
Palms in atopic individuals may reveal hyperlinear skin markings which is analogous to lichenification (Fig. 14-14)
Diagnosis
Clinical, usually straightforward
Atopic history often elicited; may also have eczema on other sites, especially the feet
Nevertheless, a diligent history must be taken to rule out contact etiology. Historical evidence of occupational and/or daily habitual exposure may be clues to the specific allergen
Patch testing with putative allergens may be performed if an allergic contact dermatitis is suspected (see Patch Testing in Appendix: Diagnostic and Therapeutic Techniques)
 Figure 14-13 Hyperkeratotic hand eczema. Scaly, itchy, erythematous plaques with painful fissures. (Image courtesy of Nejib Doss, MD.) |
 Figure 14-14 Hyperlinear palms. This is a common finding that is often noted in those with chronic atopic hand eczema. |
Management
Protective cotton-lined gloves are used for washing dishes or for other similar tasks. Vinyl or nitrile gloves should be used to avoid the risk of Latex allergy
The regular use of hand emollients, barrier creams, ointments, and avoidance of frequent contact with irritants such as soap, solvents, and detergents are the mainstays of therapy
Mild cleansers or soap substitutes are recommended
For oozing and infected lesions, compresses with Burow solution and/or mupirocin cream or ointment (Bactroban)
Because the hands and feet have a thicker stratum corneum than other areas of the body, percutaneous absorption of topical medications is decreased. Therefore, high-potency topical steroids and the use of occlusion may be needed to effectively treat inflammatory dermatoses in these sites
Class 1 to 3 topical steroids are the mainstay of treatment. Ointments penetrate the skin better than creams, but patients may prefer to use creams during the daytime and ointments at bedtime
Lower-strength (class 4 or 5) topical steroids are applied for long-term maintenance
Tacrolimus 0.1% ointment (Protopic) or pimecrolimus 1% cream (Elidel), or Crisaborole 2% ointment (Eucrisa), applied twice daily are effective as steroid-sparing agents
For severe or refractory cases, short-term administration of systemic steroids, acitretin (Soriatane), PUVA, broadband and narrowband ultraviolet B (UVB), oral cyclosporine, azathioprine, mycophenolate mofetil (CellCept), and low-dose methotrexate can also be used
Dupilumab (Dupixent) is an option for severe hand eczema resistant to other treatments
Palmoplantar Psoriasis
Lesions of palmoplantar psoriasis may involve the palms and/or soles alone, or these areas may be a part of more extensive psoriasis that is also present elsewhere on the body. The involvement of the palms and soles often presents additional problems such as pain, impairment of function, fissuring, bleeding, and embarrassment. As with chronic hand eczema (described above), palmar psoriasis runs a chronic course and is often quite difficult to manage.
Distinguishing Features
Well-demarcated erythematous plaques, with or without thick scales (Fig. 14-15)
Less likely to itch than eczema
Pustular variant is much less common (Figs. 14-16 and 14-17)
Nails may show characteristic changes (see Fingernails)
Often a positive family history of psoriasis
 Figure 14-15 Palmar psoriasis. These erythematous lesions are well-demarcated and symmetrical in distribution. |
 Figure 14-16 Palmoplantar psoriasis/palmoplantar pustulosis. Well-demarcated psoriatic plaques with multiple pustules. |
 Figure 14-17 Palmoplantar psoriasis/palmoplantar pustulosis. “Lakes of pus” in palmoplantar psoriasis. These pustules are sterile. |
Diagnosis
Clinical; psoriasis may be seen elsewhere on the body
Management
Initial Treatment
If necessary, a salicylic acid preparation such as 6% salicylic acid (Salex, Cream or Lotion) or Keralyt gel may be used to remove thick scale prior to the application of:
Potent (class 1) topical steroids for a limited period, followed by a less-potent topical steroid for maintenance
Topical steroids of a medium- or high-potency applied and then covered with vinyl or rubber gloves overnight
Maintenance Treatment
Less-potent topical steroids can be used for maintenance (e.g., triamcinolone 0.1% ointment or cream) twice daily
Topical calcitriol ointment (Vectical)
Topical calcipotriene vitamin D3 cream (Dovonex)
Topical calcipotriene and betamethasone dipropionate ointment, a vitamin D3-potent steroid combination (Taclonex ointment)
Topical calcipotriene and betamethasone dipropionate (Enstilar) foam in people 12 years of age and older
Severe, Refractory Cases
Phototherapy:
Broadband and narrowband UVB, excimer laserRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree