Hair shaft dysplasias are malformations of hair shafts. Most cases are congenital, hereditary or not; others are acquired (e.g., bubble hair). The malformations may involve a localized or generalized defect, but always follow a characteristic morphologic pattern [1,2]. The defects may be restricted to the hair or even constitute a diagnostic clue pointing to a genodermatosis (e.g., Netherton syndrome, trichothiodystrophy). Classification of hair shaft dysplasias is difficult but for practical purposes we accept the scheme shown in Table 1.1 [2,3].
Monilethrix is an autosomal dominant (AD) defect of the hair shaft characterized by short hair, only a few millimeters long and beaded. Breaking of the hair shaft occurs as soon as hair emerges from the ostium folliculorum due to narrowing of the shaft segments. Focal follicular hyperkeratosis and marked hypotrichosis may also be seen. Monilethrix generally affects individuals of different generations of the same family. The morphological defect is the periodic narrowing of the hair shaft that may be seen deep in hair follicles in biopsy specimens [4,5].
Genetics: Monilethrix is an AD hereditary defect caused by mutation of genes hHb1, hHb3, and hHb6 localized on chromosome (cr) 12q13 that encode diverse trichokeratins. We have recently reported a new family with a change in the nucleotide in heterozygosis at position 154 of exon1 of gene KRT81 (154 G > C). In the DNA sequence, this substitution involves a change of one amino acid in a protein (glycine for arginine at position 52) [6]. Interruption of keratin synthesis may be the cause of periodic variations of hair shaft diameter. Autosomal recessive (AR) cases have also been reported and are due to a gene mutation (18q) that encodes desmoglein 4 (DSG4), a situation that affects affinity for plakoglobin and alters hair shaft desmosomes [7].
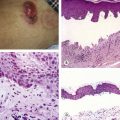
Clinical diagnosis: The clinical picture includes diffuse hypotrichosis and short, fragile, and beaded hairs. Localized (occipital region) or generalized marked follicular hyperkeratosis may also be seen (Figure 1.1).
Optical microscopy: Alternating periodical beading (defect) and knots (normal hair shaft diameter) are characteristic aspects that may also be seen in dermoscopy (Figure 1.2). The hair shaft diameter is normal in the beaded segment of the hair shaft and the medulla is observed; these are not seen in the narrowed segments.
Scanning electron microscopy: Microscopic images are similar to those observed in optical microscopy; hair shaft fracture is evidenced in narrowed segments.
Trichoscopy: Dermoscopy is a useful tool for diagnosing hair shaft dysplasias. The typical “pearl necklace” image shows elliptical beading, regularly separated by narrowing segments where hair shaft fractures are usually observed. These findings are easily identified by dermoscopy—a simple method for a quick diagnosis [8,9] (Figure 1.3).
Histology: Intrafollicular hair shaft narrowing is observed.
Classification of Hair Dysplasias
Dysplasias with Hair Fragility | Dysplasias with Little or No Hair Fragility |
Monilethrix | Pili annulati |
Pseudomonilethrix | Pseudopili annulati |
Pili torti | Diffuse woolly hair |
Menkes syndrome (kinky hair) | Woolly hair nevus |
Trichorrexis invaginata (Netherton syndrome) | Acquired progressive kinking |
Trichothiodystrophy | Diffuse partial woolly hair |
Trichonodosis | Acquired partial curly hair |
Distal trichorrhexis nodosa | Straight hair nevus |
Proximal trichorrhexis nodosa | Pili canaliculi |
Bubble hair | |
Loose anagen hair |

FIGURE 1.1 Monilethrix. Diffuse hypotrichosis in occipital region is characteristic.
Pseudomonilethrix is a rare AD defect characterized by hair fragility. Localized or diffuse hypothicosis and fake knots (irregular hair shaft flattening) occur as the result of compulsive and frequent combing of the hair. Follicular hyperkeratosis is not observed. Individuals of different generations within the same family may be affected [10,11]. This condition may be associated with trichorrexis nodosa and bubble hair.
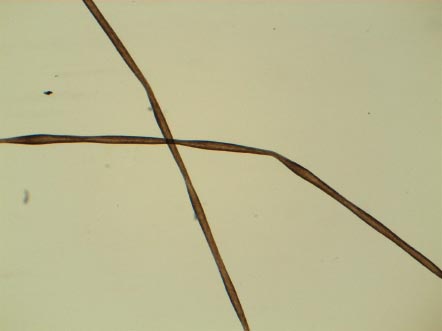
FIGURE 1.2 Typical beading with alternating knots and narrowed segments is observed.
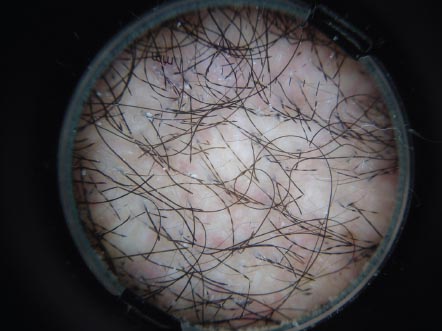
FIGURE 1.3 Elliptical beading with narrowed segments is seen on trichoscopy.
Genetics: Pseudomonilethrix is an AD defect. Specific genetic alterations have not been reported yet.
Clinical diagnosis: It is a familiar localized or diffuse hypotrichosis without follicular hyperkeratosis.
Optical microscopy: Rounded, normal appearing hairs with scarce and irregular oval or round nodules are present. Hair shaft narrowing is not observed (Figure 1.4).
Electron microscopy: What appear as nodules are actually flat segments of the hair shaft (Figure 1.5).
Trichoscopy: There are irregular distributed oval or round nodules without hair shaft narrowing segments and alternating of normal and wider segments of the hair shaft. No follicular hyperkeratosis is observed.
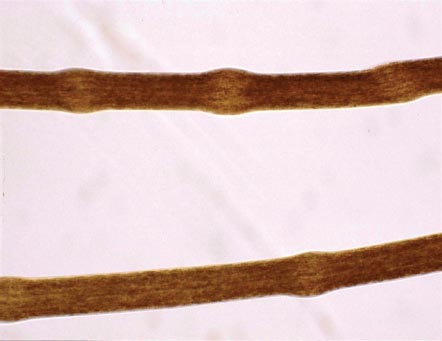
FIGURE 1.4 Pseudomonilethrix. Note round flattened nodules without hair shaft narrowing.

FIGURE 1.5 Hair shaft flattening is observed on scanning electron microscopy (SEM).
Acquired or Iatrogenic Pseudomonilethrix (Pseudopseudomonilethrix)
This defect is similar to pseudomonilethrix and arises from improper hair handling. It occurs when excessive pressure is applied to hair shafts during collection of samples from patients with monilethrix, woolly hair, and other conditions [12,13] (Figure 1.6). The same artifact is seen when a hair shaft is pressed between two slides (Figure 1.7).

FIGURE 1.6 Acquired pseudomonilethrix. The artifact in dysplastic hair is due to excessive pressure from removing hair with fingers, forceps, or tweezers.
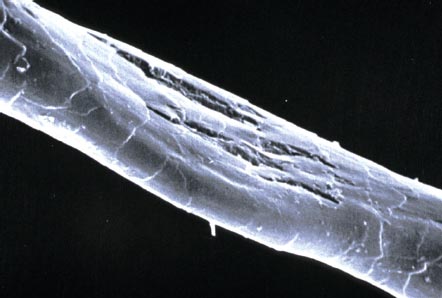
FIGURE 1.7 Another view of acquired pseudomonilethrix.
This disease involves braided hair with periodic angles about its longitudinal axis. It is an AD or AR defect that may be isolated or associated with other diseases such as Beare-Stevenson, Bazex, Crandall, Björnstad, or type 2 congenital paronychia syndromes. Atypical pili torti associated with Menkes (kinky hair) syndrome and other hair dysplasias such as pili canaliculi and woolly hair has been observed [3]. Hair appears unusually bright due to light reflection and hypotrichosis may also be observed due to oblique fractures of the hair shafts (trichoclasis) [14]. Acquired and sporadic types are also recognized [15,16].

FIGURE 1.8 Pili torti. Abundant hairs with variable bright areas appearing like sequins.
Genetics: Mutation of BSC1L (Cr 2q34–36, 2q33) is responsible for malfunctioning of adenosine triphosphatase (ATPase) involved in mitochondrial complex III synthesis, a situation that leads to oxygen-reactive species that damage sensitive ear and hair follicle cells [17]. At least this is the case in Björnstad syndrome (AD) in which neurosensorial deafness and pili torti are observed [18]. More recently, this gene has been identified in the 2 Mb region between D2S2210 and D2S2244.
Mutation of the ST14 gene (Cr 11q24.3–q.25) that encodes a protease (the matriptase type II transmembrane serine protease) has been identified in cases of pili torti associated with hypotrichosis and ichthyosis [19]. When associated with congenital hypotrichosis and juvenile macular dystrophy [20], the mutation has been identified in 16q22.1 [21]. Other mutations have been also identified in CDH3.
Clinical diagnosis: Patients usually have much hair that appears irregularly bright, depending on lighting conditions, and resembles sequins (Figure 1.8). It may be associated with localized hypotrichosis.
Optical microscopy: Braided hair with regular periodic angles is observed.
Electron microscopy: Images are similar to those observed in optical microscopy. Additionally, cuticle defects are found where steep angles occur (Figure 1.9).
Trichoscopy: Flattened hair shafts with turns at regular intervals are observed. In some cases, the defect is restricted only to a segment of the hair shaft [9]. These findings are observed more easily at ×70.
Biopsy: The same defect is observed in the hair follicles.
Associated conditions: Pili torti may be associated with nail dystrophy, ocular and teeth defects, follicular hyperkeratosis, and mental retardation.
This is a recessive, sex-liked hereditary trait due to an alteration of intracellular copper use and transfer, a condition that leads to intestinal malabsorption of the metal and consequently to low levels of copper and ceruloplasmin in plasma and organs (brain, liver, bone, elastin, hair, and skin). This syndrome is complex and involves neurological manifestations associated with hypothermia, delay in psychomotor development, limb palsies, deafness, dwarfism, hernias, and other conditions [22,23]. Affected children show peculiar faces (e.g., partridge face profile) and scarce, fine, brittle, light hair. Death takes place quickly due to neurological complications. We recently reported a case of a newborn with Menkes syndrome and transitory neonatal erythroderma [24].

FIGURE 1.9 Braided hair with cuticle defects observed under scanning electron microscopy.
Genetics: Gene ATP7A encodes a transmembrane protein that controls cellular exit of copper. A mutation of this gene is responsible for multiple sclerosis (MS) and other conditions. The gene is located on chromosomes X (Xq21.1), 4, 9 (9q31–q32), 14, and 18 (18.26.0 cM) [25,26].
Clinical diagnosis: The characteristic patient is a newborn with a peculiar partridge face. Other features are convulsions, and fine, scarce, brittle, light hair (Figure 1.10).

FIGURE 1.10 Menkes syndrome. Partridge face and poor dry hair are characteristic.
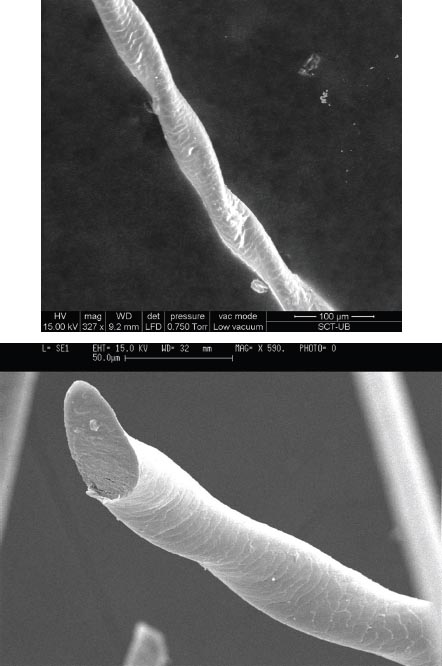
FIGURE 1.11 Atypical pili torti observed with scanning electron microscopy.
Optical microscopy: Kinky or polydysplastic hair: atypical irregular pili torti, monilethrix, and/or trichorrhexis nodosa.
Electron microscopy: Images are similar to those observed under optical microscopy (Figure 1.11). Defects of the hair cuticle are also observed, especially cuticle cells with saw aspects.
X-ray microanalysis: Low copper and sulfur contents have been reported.
Trichoscopy: Hair diameter is variable. Some segments are narrow while others look irregularly flat and twisted around their axes (atypical pili torti), a condition that may be similar to monilethrix. Irregular or atypical trichorrhesis may be found frequently.
Trichorrhexis Invaginata (Netherton Syndrome)
Trichorrhexis invaginata includes both ballooning distortions of the hair shafts and chaliced deformations of the proximal hair shaft areas. This characteristic alteration gives a hair shaft a bamboo cane appearance; therefore, this hair dysplasia is also known as “bamboo hair.” It is a specific anomaly considered a marker for Netherton syndrome, which is an AR genodermatosis observed more frequently in females. It may be associated with trichorrhesis invaginata, atopy, ichthyosis linearis circumflexa, erythroderma ichthyosiforme congenital, and ichthyosis vulgaris [3,27].
Genetics: Various gene mutations have been reported: kallikrein, corneodesmosin, desmochollin 1, desmoglein 1, transglutaminase 1, filaggrin, serine peptidase inhibitor and SPINK5 that encodes LEKTI, a serine protease inhibitor (5q.32), and NETS (5q.32) [28,29].
Clinical diagnosis: Characteristically, the affected individual is a female with ichthyosis linearis circumflexa (plaques with double squamous borders), atopy, and diffuse hypotrichosis (scarce and brittle hair) (Figure 1.12). Associated conditions are ichthyosis vulgaris or erythroderma ichthyosiforme congenita. Trichothiodystrophy may also be associated to ichthyosis, a condition that should be ruled out.
Optical microscopy: Bamboo hair (trichorrhesis invaginata) is a typical image, It is a ballooning deformity of the hair shaft that lies in a proximal chaliced-shaped area. Eyebrows and eyelashes may be also affected.
Electron microscopy: The images are similar to those observed by an optical microscope (Figure 1.13). Hair shaft distal ends may appear as a golf poles due to hair fractures at the knots of trichorrhexis invaginata.
Trichoscopy: Hairs are fractured at the nodules or knots where a shaft appears as a bamboo cane knot. Typical aspects are chaliced shapes of the proximal ends and ballooning distortions of the distal parts of knots. Distal ends of hair shafts show a golf pole aspect due to local fracture [30,31].

FIGURE 1.12 Trichorrhexis invaginata (Netherton disease). Girls with scarce, poor, dry hair usually present with ichthyosis linearis circumflexa characterized by squamous double borders. (Courtesy of Prof. P. de Unamuno.)

FIGURE 1.13 Typical “bamboo hair” with proximal dilatation of the hair shaft into chalice-shape distortion and distal ballooning alteration.
Trichothiodystrophy (TTD) is a complex syndrome caused by low levels of sulfur compounds in the hair that lead to a specific dysplasia known as trichodystrophic hair [1,3,32]. The syndrome is associated with other clinical findings such as a delay in psychomotor development, ichthyosis, onycodystrophy, micro-dolicocephalia, photosensitivity, and other defects [33,34]. Some variations of the syndrome include BIDS (Brittle hair, Intellectual impairment + Decreased fertility and Short stature or Amish brittle hair syndrome or TTD type D), IBIDS (Ichthyosis or Tay syndrome or TTD type E), PIBIDS (Phosensitivity or TTD type F), SIBIDS (+osteoSclerosis, ONMRS or Itin syndrome), and syndromes of Sabinas (TTD type B, with nail dystrophy) and Pollit (TTD type C, + neonatal retardation). The term TTD type A is reserved for when only the isolated congenital hair defect is present.
Genetics: Mutations of TTD, ERCC2, C7orf11, ERCC3, GTF2H5, XPC, and GTF2H4 genes localized in 19q13.2–q13.3, 19q13.3, 7p14.1, 2q21, 6q25.3, 3p25, and 6p21.3, respectively, have been reported [37–39].
Clinical diagnosis: The affected individual is a newborn with congenital ichthyosis, scarce, short, and brittle hair, and a characteristic face: microdolicocephalia and pleasant appearance (Figure 1.14). Other clinical findings may include mental retardation, growth delay, onycodystrophy (nail striae), and photosensitivity [33].
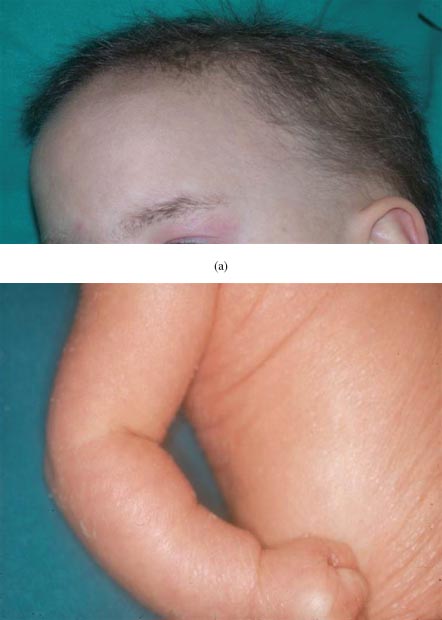
FIGURE 1.14 Trichothiodystrophy: (a) scarce, short, brittle hair with microdolicocephalia and (b) ichthyosis.
Optical microscopy: Flat hair appears with typical transverse and clean transversal fractures (trichoschisis); see Figure 1.15a.
Polarized light: Alternating light and dark bands in the hair presenting a typical spotted tiger-like surface are observed; see Figure 1.15b.
Scanning electron microscopy: Completely rigid flat hairs that resemble tapes are observed. Trichoschisis with a clean fracture is pathognomonic. The hair surface shows longitudinal crests and cuticle defects (Figure 1.16).
X-ray microanalysis: Sulfur content is lower than 50% (Figure 1.17).
Amino acid chromatography: Hair-sulfured amino acids are clearly lowered.
Trichoscopy: Dermoscopy is not characteristic except for the trichoschisis [40]. Hair shafts may also show weaving contours and non-homogeneous structures such as grains of sand, alternating dark and light bands, and spotted tiger-like surfaces.

FIGURE 1.15 Trichothiodystrophy: (a) Flat hair with typical transverse fractures (trichoschisis) and (b) characteristic spotted tiger tail-like appearance.
This is a frequent but rarely diagnosed hair dysplasia in which true knots are observed along the hair shafts. It may be suspected when hair shafts show angles and abruptly change their directions [2,41]. This condition is more frequently observed in individuals with curly hair in association with local trauma, scraping maneuvers, and tics [42]. It may be found in the armpit and genitalia in association with pediculosis and acarophobia. How the double or even more complex knots are originated is not yet completely understood.
Clinical diagnosis: Trichonodosis usually occurs as an isolated finding. Suspicions may arise when a hair abruptly changes its direction due to a true knot.
Optical microscopy: A simple, double, or even complex true knot (“tie knot”) is observed (Figure 1.18).
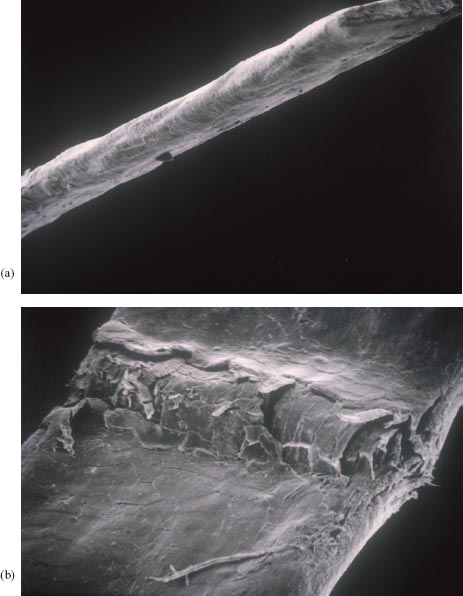
FIGURE 1.16 Trichothiodystrophy: Scanning electron micrographs of (a) flat hair resembling tape and (b) initial trichoschisis.
Scanning electron microscopy: Similar images to those observed by optical microscopy are seen. Amplification may reveal cuticle defects in the true knot area (Figure 1.19).
Trichoscopy: A simple, double, or complex true knot is observed. Sometimes a “tie knot” or a “sailor knot” is observed in dermoscopy.
Trichorrhexis nodosa is defined as the presence of nodules of fracture on hair shafts. Clinical findings differ, depending whether the fracture occurs proximally or distally in the shaft [2,42]. Alopecia is observed only in the former case.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


