This chapter considers a series of changes of hair due to color (e.g., green hair) or loss (alopecia) including cicatricial (tufted folliculitis) and non-cicatricial (alopecia areata, trichotillomania) forms that occur primarily during childhood and adolescence. We do not consider more common processes that are diagnosed easily, for example, androgenic alopecia or telogen and anagen effluvium. For further information on these processes, readers can consult the textbook by Camacho and co-workers [1] or the review of Moreno-Romero and Grimalt [2]. Deficient hair losses caused by nutritional or metabolic disorders are not addressed either. Finally, the descriptions include infrequent clinical patterns such as alopecia parvimaculata and bird’s nest hair.
Hair development begins in utero at the ninth week with the formation of follicular units composed of epidermally derived follicles and mesodermally derived papillae [3]. Primary hair follicles first develop on the eyebrows, upper lip, and chin. They later develop over the scalp in a frontal-to-occipital direction and over the body in a cephalocaudal direction. Secondary follicles then form at the sides of the primary follicles, producing typical groups of three hairs on a follicular unit. At 16 weeks’ gestation, hair production begins in the follicles. All follicles produce lanugo hair that grows 2 to 3 cm in length [4]. Fine lanugo hair covers the scalp and appears elsewhere in a cephalocaudal direction, eventually covering the entire fetus. This constitutes the first anagen (growth) wave. At 26 to 28 weeks’ gestation, the body and most of the scalp hair follicles enter catagen and subsequent telogen phases in a programmed wave in a cephalocaudal direction in the body and a frontal-to-parietal direction on the scalp. Most of these telogen hairs are shed in utero [5], although this may be delayed until after birth. A band-like area of occipital hair does not enter telogen until 8 to 12 weeks after birth. These occipital hairs fall out, producing a well-defined area of alopecia known as occipital alopecia of the newborn at 4 to 8 months of age [6]. This process has been renamed transient neonatal hair loss (TNHL) [7].
The duration of growth of the scalp hairs extends, while the duration of body hair growth shortens to produce hairs 1 cm in length. These second body hairs grow for 4 to 8 weeks, then enter telogen, and are shed during the first 3 or 4 months of life and are replaced by a third coat of hair. Body hairs progressively shorten into vellus hairs, most of which do not protrude from follicles. Scalp hair enlarges progressively with each cycle into terminal hair. Some infants display intermediate hair from 3 months until the age of 2 years. This hair is coarser than lanugo hairs, but still sparsely pigmented [8].
At full term of a pregnancy, the scalp reveals two consecutive waves of hair, each running from forehead to occiput. Toward the end of the first year of life, after development of the first two synchronized waves of telogen, the scalp undergoes a transition to a random mosaic pattern in which each hair has its own intrinsic rhythm. This asynchrony continues throughout life unless modified by pregnancy or illness.
Clinical diagnosis: A band-like area of occipital hypotrichosis appears until 8 to 12 weeks after birth: the occipital alopecia of the newborn is seen around 4 to 8 months of age (Figure 3.1).
Treatment: Spontaneous regrowing of hair is usual.

FIGURE 3.1 Transient neonatal hair loss with characteristic band-like hypotrichosis of the occipital area.
Focal and Multifocal Alopecia Areata
Alopecia areata (AA) is a chronic follicular inflammatory process of autoimmune origin that leads to interruption of the follicular cycle during an early phase of anagen with detachment of telogen hairs. Therefore, when the cause is no longer active, recovery is complete after an extended time (months or even years) has passed. AA appears in the form of one or several rounded, well-defined plaques of non-cicatricial alopecia that may evolve into alopecia totalis or alopecia universalis. Focal AA consists of localized forms of AA consisting of one or several plaques (multifocal AA) of ophiasic distribution around temporal and occipital areas.
Short hairs on the borders of the plaques measuring a few millimeters in length, thicker at the distal ends (“exclamation mark or peladic hairs”), are pathognomonic as are the “cadaveric” hairs seen as black points. These types of hairs indicate that the process is active and the plaques will extend even further. When recovery begins, fine white vellus hair is observed in the centers of the plaques.
AA is a frequent finding (approximately 2% of dermatological consultations) of familial incidence (in at least 25% of cases). It commonly begins in childhood and 60% of patients are under 20 years old. AA is chronic and relapsing, and involves several etiopathogenic factors such as foci of infections, stress, and presence of immune complexes or autoantibodies over a genetic base. Association with immunological disorders is frequent, especially with autoimmune thyroiditis, celiac disease, atopy, Down syndrome, vitiligo, and others [9]. In some of these disorders, evolution is chronic and the prognosis is poor.
We must also bear in mind that AA can affect the nails, and in cases of trachyonychia, the appearance of the nail plate is rough. An exceptional clinical pattern in children is the diffuse form of AA. It must be considered when diffuse acute alopecia is observed [10].
Clinical diagnosis: One or several rounded, well-defined plaques of non-cicatricial alopecia may show “exclamation mark hairs” (Figure 3.2) on their borders. These plaques develop chronically and tend to converge in ophiasic patterns in temporal areas. In the acute diffuse type of AA, peladic hairs are useful signs for supporting such a diagnosis. A differential diagnosis should consider congenital alopecia triangularis, alopecia parvimaculata, and trichotillomania.
Light microscopy: The peladic hairs or hairs that are easily detached from the plaque borders are of the telogen type (Figure 3.2).
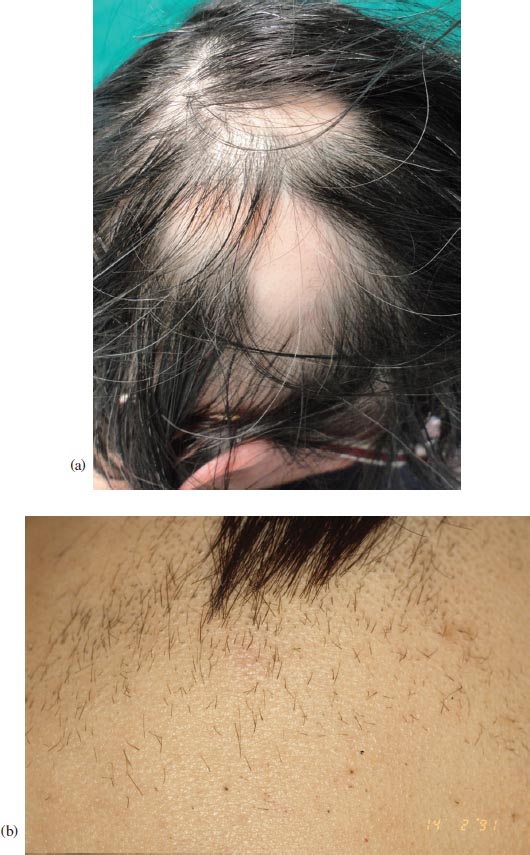

FIGURE 3.2 Multifocal alopecia areata. (a) Typical plaques of alopecia areata showing non-cicatricial rounded aspects. (b) Multiple peladic hairs on margins of plaques. (c) Detail of initial formation of peladic (“exclamation mark”) hair: telogenic root and distal end with wider diameter.
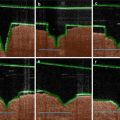
Dermoscopy: Peladic and “cadaveric” hairs (black dots) and lighter color dots that correspond to prominent sebaceous glands in empty follicles on the skin surface can be seen (Figure 3.3).
Histology: Biopsy of active borders of plaques shows moderate round cell peribulbar inflammatory infiltrate (Figure 3.4). A study with monoclonal antibodies shows that this infiltrate consists mostly of T-helper lymphocytes.
Treatment: The etiopathogenesis of AA has not been clarified completely. Several treatments may be helpful although individual responses to their use are quite variable. To ensure that side effects are reduced to a minimum, we suggest establishment of a scale that classifies treatments based on their levels of aggressiveness, while considering the patient’s degree of complaint.

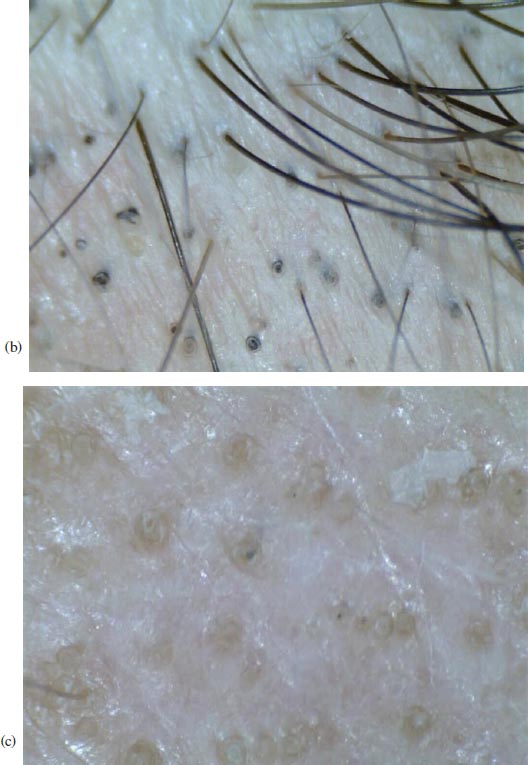
FIGURE 3.3 Trichoscopy results: (a) characteristic “exclamation mark hairs”; (b) black dots (cadaveric hairs); and (c) lighter dots representing empty hair follicles.
In localized focal forms of AA (plaques, for example), we recommend local rubefacients only. In this phase, the plaques often undergo spontaneous involution. In multifocal AA, more aggressive treatments are usually necessary: 1 to 2% dithranol locally for short contact therapy or 2 to 3% minoxidil plus clobetasol propionate 0.025 to 0.050% topical solution (Figure 3.5) [11]. The oral administration of 10 mg per day of biotin may be helpful. In severe cases, steroid pulse therapy can be used [12]. Local sensitization with diphencyprone or dinitrochlorobenzene (DNCB) and steroid treatment is not recommended in children.
Alopecia Areata Totalis and Universalis
Alopecia areata totalis is an AA that affects the scalp. AA universalis affects all hair follicles of the body including eyebrows and eyelashes. Both forms are related to the extreme evolution of AA, although they may begin with acute, diffuse forms. These generalized forms of AA are often associated with processes that have immunological bases, especially Hashimoto’s thyroiditis, and others such as pernicious anemia, vitiligo, myasthenia gravis, and celiac disease in children [13]. Many patients are atopic, and in half of the cases the possibility of regrowth is not especially favorable. AA should be studied following a standardized assessment protocol such as that proposed by Olsen et al. [14].
Clinical diagnosis: Children, youths, and adults may be affected by chronic acquired alopecia totalis or alopecia universalis (Figure 3.6) developed from AA in plaques or rarely from acute diffuse AA. These alopecias may affect several members of the same family or community. Some advanced cases of alopecia totalis involve the entire area of the scalp with the exception of isolated hairs on the borders of the scalp and vertex. This condition may be accompanied by trachyonychia (Figure 3.7) or associated with immunological diseases. A differential diagnosis must consider atrichias and hypotrichoses (congenital alopecias) [14].
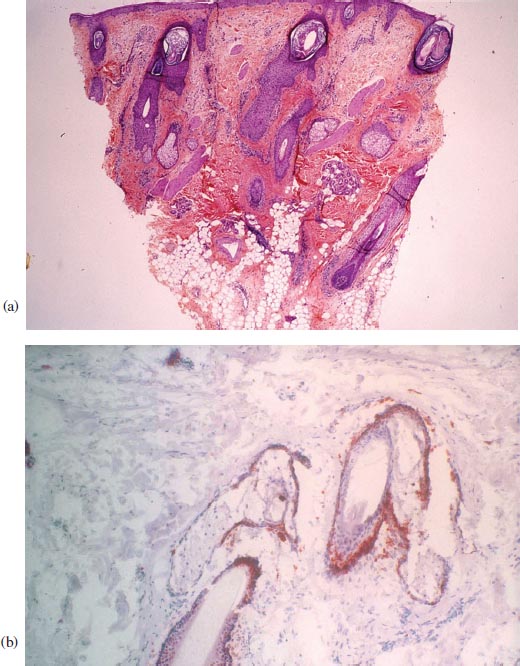
FIGURE 3.4 Histopathology: (a) perifollicular peribulbar infiltrate (POF); (b) characteristic CD4 positive.

FIGURE 3.5 New hair appears after short contact dithranol therapy.
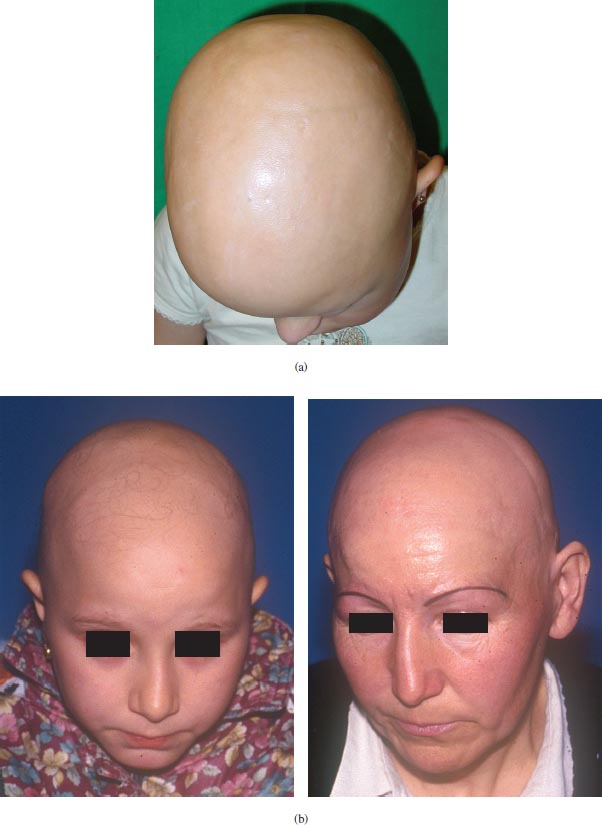
FIGURE 3.6
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


