Abstract
Glucocorticoids are among the most commonly utilized topical, intralesional, and systemic therapies for cutaneous diseases. A thorough understanding of their mechanisms of action, formulations, administration, and potential adverse effects enables dermatologists to effectively and safely treat patients with this indispensable class of medications.
Keywords
corticosteroids, intralesional corticosteroids, topical corticosteroids, systemic corticosteroids, glucocorticoids, prednisone, hypothalamic–pituitary–adrenal (HPA) axis, adrenal suppression, glucocorticoid toxicity, corticosteroid withdrawal syndrome
- ▪
Glucocorticoids continue to be among the most commonly prescribed anti-inflammatory agents in dermatology and all of medicine, with a large number of disorders responding to these drugs
- ▪
Proper use of systemic glucocorticoids requires a working knowledge of the hypothalamic–pituitary–adrenal (HPA) axis
- ▪
Proper use of topical and intralesional glucocorticoids requires awareness of their various formulations and potencies
- ▪
Glucocorticoids have a broad range of potential adverse effects that can be minimized by a variety of strategies
- ▪
Clinical usage guidelines facilitate proper dosing and administration of glucocorticoids for both short- and long-term therapy
Introduction
The Nobel Prize in Medicine was awarded in 1950 to Hench and associates for their initial work on the beneficial effects and toxicities of corticosteroids for rheumatic disorders. In 1951, Sulzberger and colleagues first reported the use of systemic cortisone and adrenocorticotropic hormone (ACTH) as therapies for inflammatory skin diseases. One year later, Sulzberger and Witten successfully treated eczematous eruptions with topical hydrocortisone. A novel method of high-dose glucocorticoid therapy was introduced to dermatology in 1982 by Johnson and Lazarus , who used pulse intravenous therapy for pyoderma gangrenosum. During the past 40 years, a variety of other anti-inflammatory/immunomodulatory drugs have been developed, allowing for a “corticosteroid-sparing” effect and minimization of risks from long-term therapy with systemic glucocorticoids.
Pharmacology and Mechanism of Action
Structure and Metabolism
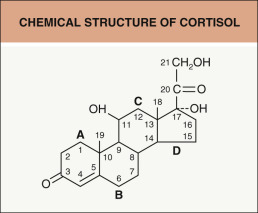
All steroids, including glucocorticoids, have the basic four-ring structure of cholesterol, with three hexane rings and one pentane ring. Fig. 125.1 shows the chemical structure of hydrocortisone (cortisol). Modifications in the basic four-ring structure of glucocorticoids result in systemic agents that have different potencies, mineralocorticoid effects, durations of action (biologic half-life), and metabolism; these agents are commonly referred to as corticosteroids, and this term is used elsewhere in the book. Table 125.1 lists the key pharmacologic properties of the major systemic agents used today. Similar changes in the basic structure of the glucocorticoid molecule have resulted in various topical agents with differing solubilities, lipophilic properties, degrees of percutaneous absorption, and glucocorticoid receptor-binding activities. Table 14.11 defines glucocorticoid structural classes relevant for allergic reactions and cross reactivity among agents.
| PHARMACOLOGY OF SYSTEMIC GLUCOCORTICOIDS (GCs) | |||||
|---|---|---|---|---|---|
| Equivalent GC dose (mg) | GC potency (relative) | Mineralocorticoid potency (relative) | Duration of action (hours) * | Plasma half-life (minutes) | |
| Short-acting | |||||
| Cortisone | 25 | 0.8 | 1.0 | 8–12 | 60 |
| Hydrocortisone | 20 | 1 | 0.8 | 8–12 | 90 |
| Intermediate-acting | |||||
| Prednisone | 5 | 4 | 0.25 | 24–36 | 60 |
| Prednisolone | 5 | 4 | 0.25 | 24–36 | 200 |
| Methylprednisolone | 4 | 5 | 0 | 24–36 | 180 |
| Triamcinolone | 4 | 5 | 0 | 24–36 | 300 |
| Long-acting | |||||
| Dexamethasone | 0.75 | 25–30 | 0 | 36–54 | 200 |
| Betamethasone | 0.6 | 30–35 | 0 | 36–54 | 200 |
When examining the chemical structure of glucocorticoids, it is important to recognize that active agents such as hydrocortisone (see Fig. 125.1 ) have a hydroxyl group at the 11 position. The corresponding inactive drug, cortisone, has a ketone group at the 11 position and must undergo hepatic conversion to hydrocortisone for biologic activity. The same is true for prednisone, which must undergo the identical 11-hydroxylation by the liver to produce an active agent, prednisolone. Since conversion of the inactive drug to its active analogue is impaired in patients who have severe hepatic disease, it is best to treat such individuals with a medication such as prednisolone that does not require metabolic alteration to be of therapeutic benefit .
In addition to indicating equivalent glucocorticoid doses in milligrams, Table 125.1 shows that these agents differ in their relative mineralocorticoid as well as glucocorticoid potencies. Cortisone and hydrocortisone have fairly significant mineralocorticoid potency, whereas prednisone and prednisolone have slight mineralocorticoid effects. A drug that has no mineralocorticoid activity, such as methylprednisolone, would be most appropriate in situations where mineralocorticoid effects must be avoided .
Plasma half-lives of the various systemic glucocorticoids vary from about 1 to 5 hours, as seen in Table 125.1 . However, the plasma half-life is a poor indicator of the duration of action (biologic activity) of each drug. Duration of biologic effect is best assessed by the period of suppression of ACTH secretion from the pituitary gland after the administration of a single dose of a particular glucocorticoid. As indicated in Table 125.1 , short-acting glucocorticoids have an effect for 8–12 hours, intermediate-acting agents for 24–36 hours, and long-acting agents for more than 48 hours. Duration of biologic activity is a critical factor in choosing a glucocorticoid for alternate-day therapy. Intermediate-acting agents should be used for this purpose, with long-acting agents avoided because there would be no period for recovery of the hypothalamic–pituitary–adrenal (HPA) axis (see below) .
Absorption and Distribution
Oral glucocorticoids are absorbed in the jejunum, with peak plasma levels occurring 30–90 minutes after intake. Administration of these drugs with food may delay absorption but does not decrease the amount absorbed.
Once glucocorticoids reach the plasma, the primary carrier protein is corticosteroid-binding globulin (CBG), also known as transcortin. Most endogenous cortisol is bound to CBG, and low doses of exogenous glucocorticoids are primarily bound by this high-affinity, but low-capacity, carrier system. With higher glucocorticoid doses, some binding also occurs to albumin in a low-affinity fashion, but with a greater capacity because of the larger amount of albumin in plasma. The avidity with which exogenous glucocorticoids bind to these two carrier proteins is less than that of endogenous cortisol. As exogenous glucocorticoids fill CBG binding sites, an increase in low-affinity binding to albumin leads to a greater fraction of free (unbound) glucocorticoid. This free fraction is biologically active, entering cells and mediating glucocorticoid effects . Disorders that result in decreased binding proteins in the plasma, such as hepatic or renal disease, increase the free fraction of exogenous glucocorticoids and thereby augment the therapeutic effects and toxicities of these drugs.
The Hypothalamic–Pituitary–Adrenal (HPA) Axis
A working knowledge of the normal function of the HPA axis is required to understand glucocorticoid physiology. The hypothalamus produces corticotropin-releasing hormone, which is released in small pulses into the pituitary circulation. The anterior pituitary responds to corticotropin-releasing hormone with synthesis of ACTH and its subsequent pulsatile secretion into the peripheral circulation. ACTH is the hormone that stimulates the middle layer of the adrenal cortex to generate and release cortisol. In an individual with a normal sleep cycle, the greatest amount of cortisol is released during the early morning hours prior to waking. Under basal conditions, the adrenals produce approximately 20–30 mg of cortisol (equivalent to 5–7.5 mg of prednisone) per day in an adult, but this may increase up to 10-fold under times of maximal stress. ACTH also has some role in stimulating adrenal androgen production, but it is not significantly involved in the production of the major mineralocorticoid, aldosterone. The major mineralocorticoid control mechanisms are the renin–angiotensin system and serum potassium levels.
There are three main control mechanisms for endogenous cortisol secretion . The first is a negative feedback effect by plasma cortisol, which inhibits the secretion of corticotropin-releasing hormone and ACTH by the hypothalamus and pituitary, respectively. The second method of regulation is the pulsatile secretion of ACTH, which is based on a circadian cycle, with increasing pulses beginning several hours after the onset of sleep and reaching a maximum shortly before waking. From these ACTH pulses, the peak release of cortisol in a typical sleep cycle is at about 6–8 a.m. With other sleep cycles, the circadian pattern will adjust so that peak cortisol levels occur just prior to waking. The third form of control of endogenous cortisol production comes from neural effects on the HPA axis in response to various emotional or physical stresses. These neural stimuli include catecholamine production from the brainstem, corticotropin-releasing hormone from sites other than the hypothalamus, and vasopressin.
Molecular Mechanisms
As depicted in Fig. 125.2 , the glucocorticoid free (unbound) fraction enters cells and exerts its effects by binding to a cytoplasmic glucocorticoid receptor, which is within a protein complex that includes heat shock proteins . Binding of glucocorticoids to this receptor leads to their translocation into the nucleus and eventual release from the protein complex. In the nucleus, the glucocorticoid receptor forms a dimer that binds to glucocorticoid response elements in the promoter region of certain genes (see Fig. 125.2 ). Approximately 10–100 genes in each cell are regulated directly by glucocorticoids . This binding affects the rate of transcription, inducing or (less often) repressing specific messenger RNA production and protein synthesis.
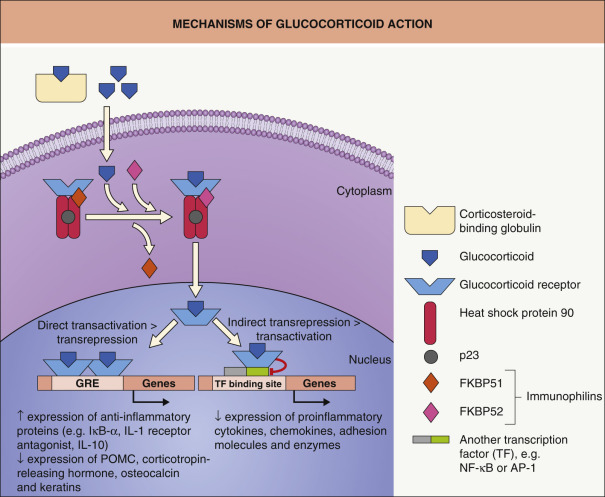
The glucocorticoid receptor also interacts with other transcription factors (see Fig. 125.2 ) that have a central role in the inflammatory response as well as their coactivator molecules, such as cAMP response element binding protein (CREB)-binding protein. Nuclear factor-κB (NF-κB) is an important transcription factor that induces the expression of many genes that play a significant role in chronic inflammation, encoding various cytokines, adhesion molecules, inflammatory enzymes, and growth factors. By indirectly and directly inhibiting NF-κB, the glucocorticoid receptor can dramatically reduce the inflammatory process . The glucocorticoid receptor also has an inhibitory effect on activator protein 1 (AP-1), a heterodimeric transcription factor composed of proteins such as c-jun, c-fos, and activating transcription factor; this likewise controls expression of growth factor and cytokine genes. The key cytokines and other proinflammatory molecules that are inhibited by glucocorticoids and the effects of these drugs on inflammatory cells are summarized in Table 125.2 .
| ANTI-INFLAMMATORY EFFECTS OF GLUCOCORTICOIDS |
| Decreased production of cytokines and other proinflammatory molecules |
|
| Effects on inflammatory cells |
|
Clinical Indications, Dosages and Contraindications
Table 125.3 lists major categories of dermatologic disease where systemic glucocorticoids are used. There are many more skin conditions for which topical and intralesional glucocorticoids can be helpful, such as eczematous and papulosquamous disorders and other localized inflammatory processes.
| MAJOR USES OF SYSTEMIC GLUCOCORTICOIDS IN DERMATOLOGY |
| Severe dermatitis |
|
| Bullous dermatoses |
|
| Vasculitis |
|
| Autoimmune connective tissue diseases |
|
| Neutrophilic dermatoses |
|
| Other disorders |
|
Oral Therapy
Dermatologists use glucocorticoids for short periods to treat acute conditions such as extensive allergic contact dermatitis and other acute eczematous disorders. Therapy is considered short-term if it is administered for approximately 3 weeks or less. If a skin disease requires a longer course of therapy (months to years), the addition of a glucocorticoid-sparing agent should be considered to assist in reducing the dosage and duration of glucocorticoid therapy. An oral agent with an intermediate duration of action, such as prednisone, is usually given in a single early-morning dose to achieve the least HPA axis suppression. In some severe acute dermatoses, the dose can be divided and administered twice daily for better initial control (versus more frequent intravenous administration), but conversion to a single early-morning dose should occur as soon as possible. Split-dose therapy results in parallel increases in efficacy and toxicity. The total number of milligrams given daily as a split dose is considered to be biologically equivalent to a slightly higher single morning dose. The daily dose of prednisone varies depending on the severity of the dermatosis, but for most moderate conditions, a common initial dose is 40–60 mg/day in average-weight adults or approximately 1 mg/kg/day in children.
Prednisone is often the intermediate-acting glucocorticoid of choice for both short- and long-term therapy. It is inexpensive and available in many dosage forms . Methylprednisolone can be used if there is a need to avoid any mineralocorticoid effects. Intermediate-acting drugs such as prednisone and methylprednisolone are also utilized for alternate-morning therapy (a common component of tapering regimens; see below), which allows the HPA axis to recover in the last 12 hours of the off-day of therapy. Other advantages of alternate-morning glucocorticoid therapy are listed in Table 125.4 . Two important side effects of long-term glucocorticoid therapy that are not minimized by alternate-morning dosing are osteoporosis and cataracts (see below).
| ALTERNATE-MORNING GLUCOCORTICOID THERAPY |
|---|
|
Although it may help to prevent a disease rebound, tapering of the glucocorticoid dose is not usually necessary from an adrenal recovery standpoint with short-term therapy. However, tapering to allow adrenal recovery is an important consideration when treatment is for longer than 3–4 weeks, especially at a dose ≥20 mg/day (see HPA Axis Suppression below). Even in the absence of overt adrenal insufficiency, patients can develop a glucocorticoid withdrawal syndrome characterized by arthralgias, myalgias, mood changes, fatigue, headache, nausea, and anorexia . When this occurs, a return to the previous dose of glucocorticoid, followed by more gradual tapering, is recommended. In general, the rate of prednisone tapering depends on both features of the dermatosis (e.g. type, activity, severity) and adrenal recovery issues. The prednisone dose can usually be tapered in 20 mg increments at doses greater than 60 mg/day, 10 mg increments between 30 and 60 mg/day, and 5 mg increments between 30 mg and the physiologic dose range. Once the physiologic dose range of 5–7.5 mg/day of prednisone is reached, a more gradual reduction (e.g. in 1–2.5 mg increments) may be necessary to allow adrenal recovery.
Another method of glucocorticoid dosage tapering is to convert from daily to alternate-day therapy once the prednisone dose is about 20–30 mg/day . The simplest way to convert is to multiply the previous daily dose by 2–2.5 times for the on-day dose, and taper therapy rapidly on the off-day. An alternative method is to increase the on-day dose by 5 mg increments and decrease the off-day dose by a similar amount, until therapy is eventually doubled on the on-day and stopped on the off-day. Finally, simultaneous tapering and alternate-morning conversion can be accomplished by decreasing the dose by 5 mg on the alternate morning, with the patient eventually taking the same dose every other morning as they were taking daily.
Intramuscular Therapy
Dermatologists occasionally use intramuscular administration of glucocorticoids for control of acute dermatoses . Although some acute dermatoses respond very well to intramuscular glucocorticoid therapy, serious conditions such as pemphigus vulgaris or SLE are best treated by other routes of systemic administration because of the initial need for higher daily doses and the requirement for more control over dosage changes. Advantages of intramuscular glucocorticoid therapy include guaranteed compliance due to physician administration and an assured steady release of glucocorticoids from the injected depot preparation. Critics of intramuscular therapy stress that oral morning doses are more physiologic, are absorbed more predictably, allow more precise tapering, and can be administered on alternate-morning schedules to decrease HPA axis suppression. There is also the possibility of lipoatrophy or a sterile abscess at an injection site, especially with triamcinolone, if the injection is not given deeply enough into the muscle. Intramuscular agents such as betamethasone and dexamethasone, which have a duration of action of less than 1 week, may be preferred in self-limited dermatoses. Longer-acting intramuscular agents that produce effects for about 3 weeks, such as triamcinolone acetonide and methylprednisolone acetate, should not be given more than about four to six times per year. The physician might be lulled into thinking that therapy is intermittent and relatively safe, while in fact it is continuous for ≥3 weeks per injection, necessitating time for HPA axis recovery.
Intravenous and Pulse Therapy
Intravenous doses of glucocorticoids may be necessary in life-threatening dermatologic conditions. A total daily dose of 2 mg/kg or more of methylprednisolone is given initially in divided doses every 6–8 hours in these acute and critical situations. Another method of dosing glucocorticoids in severe dermatologic disease is intravenous pulse therapy . With this method, methylprednisolone is given intravenously in doses of 0.5–1 g over 2 hours daily for 1–5 days. This therapy was formerly given in an inpatient setting with cardiac monitoring because arrhythmias and rare cases of sudden death are possible if rapid administration results in acute electrolyte shifts. However, coadministration of potassium helps to avoid this problem, and slow infusion of the methylprednisolone over 2 hours usually prevents cardiac effects, allowing use of this therapy in an outpatient setting. Most commonly, oral doses are continued on a maintenance basis after pulse therapy is given. Pulse therapy allows for a dramatic acute effect in severe dermatoses, but hopes that it would greatly reduce the need or dose of maintenance therapy have not been realized.
Topical Therapy
For topical glucocorticoid therapy, there are many different medications available in a wide range of potencies and a variety of vehicles. Topical glucocorticoids have been categorized by the WHO into four major potency groups that span seven classes, ranging from the ultra high potency agents in class 1 to the very low potency agents in class 7. These classes have been developed based on vasoconstrictor assays and double-blind clinical studies. Investigators graded the intensity of cutaneous vasoconstriction within normal skin of control subjects after overnight application of various agents and found significant correlation between degree of vasoconstriction and clinical efficacy (response of psoriatic lesions treated for 2–3 weeks) . A list of topical preparations in each class is shown in Table 125.5 . The vehicle can greatly influence the percutaneous absorption and therapeutic efficacy of a particular glucocorticoid. In some instances, brand-name and generic formulations of the same agent, concentration, and vehicle type may have different potencies (see Table 124.3 ). As a result, in the era of generic substitutions and limited formularies, the clinician needs to consider these points, as well as non-adherence, as potential explanations for an unresponsive dermatosis.
| POTENCY RANKING OF SOME COMMONLY USED TOPICAL GLUCOCORTICOIDS | ||
|---|---|---|
| WHO potency group | Class | Topical glucocorticoid agent and formulation |
| Ultra high (super-potent) | 1 |
|
| High | 2 |
|
| 3 | ||
| Moderate (medium) | 4 |
|
| 5 |
| |
| Low | 6 |
|
| 7 |
| |
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


