Generalized Eruptions
OVERVIEW
There are drug eruptions, viral and bacterial exanthems that can become widespread and occasionally life-threatening. Erythema multiforme major (Stevens-Johnson syndrome), toxic epidermal necrolysis, and exfoliative dermatitis (erythroderma) may produce generalized eruptions and present as medical emergencies. Staphylococcal scalded skin syndrome (SSSS), however, has a generally benign outcome with a very low mortality.
Erythema multiforme major, also known as Stevens-Johnson syndrome (SJS), and toxic epidermal necrolysis (TEN) are now believed to be variants of the same condition on a spectrum of clinical presentations and are often referred to as “SJS/TEN.” They are discussed separately in this chapter because of several of their unique cutaneous manifestations.
Staphylococcal Scalded Skin Syndrome
Staphylococcal scalded skin syndrome (SSSS) is primarily a disease of children and neonates. Also known as Ritter disease, SSSS includes a spectrum of superficial blistering skin disorders caused by the hematogenous spread of exfoliative toxins type A or B of Staphylococcus aureus. It is a syndrome of acute exfoliation of the skin. Severity varies from a few blisters localized to the site of infection to a severe exfoliation affecting almost the entire body.
SSSS is characterized by red blistering skin that looks like a burn or scald, hence its name. Children are believed to be more at risk because of lack of immunity and immature renal clearance capability (exfoliative toxins are renally excreted). Maternal antibodies transferred to infants in breast milk are thought to be partially protective, but neonatal disease can still occur, possibly as a result of inadequate immunity or immature renal clearance of exotoxin.
The exotoxins from S. aureus produce a red rash and separation of the epidermis beneath the granular cell layer (intraepidermal), which differs from the more severe toxic epidermal necrolysis (TEN) wherein the cleavage site involves necrosis of the full epidermal layer (see below).
Bullae form, and diffuse sheet-like desquamation occurs. Outbreaks are usually due to infection picked up from asymptomatic carriers in neonatal and newborn nurseries. Reports implicating methicillin-resistant S. aureus (MRSA) and community-acquired MRSA as a cause of SSSS are increasing.
Distinguishing Features
SSSS presents as an erythematous rash followed by diffuse epidermal exfoliation characterized by the appearance of large fluid-filled flaccid bullae that rupture easily, leaving an area that looks like a burn (Figs. 20-1 and 20-2).
Fever, although patients may be afebrile; in fact, most patients do not appear severely ill
Tenderness and warmth on palpation
Nikolsky sign: gentle stroking of the skin results in a separation of the epidermis at the dermal-epidermal junction resulting in the dislodgement of intact superficial epidermis
Exfoliation may be patchy or sheet-like in nature
Facial edema
Perioral crusting
Dehydration may be present and significant
 Figure 20-1 Staphylococcal scalded skin syndrome (SSSS). Diffuse erythema and sloughing of the skin. |
 Figure 20-2 Staphylococcal scalded skin syndrome (SSSS). Folds of the body are usually the first to exfoliate. |
Diagnosis
Suspected from the characteristic history and physical examination
May be confirmed with a biopsy and bacterial culture taken from the eyes, nose, or umbilicus. The bacteria are not present in the skin lesions, as these are due to the action of an exotoxin.
Management
Treatment usually requires hospitalization. Intravenous antibiotics are generally necessary to eradicate the staphylococcal infection
Maintenance of fluid and electrolyte balance
Strict handwashing with antibacterial soap
Exfoliative Dermatitis (Erythroderma)
Exfoliative dermatitis (ED), also referred to as erythroderma, is a generalized scaling eruption with a marked loss of exfoliated epidermis due to an increased mitotic rate. At its peak, ED may involve more than 90% of the cutaneous surface. It may arise idiopathically or secondary to an underlying cutaneous or systemic disease or as a reaction to a drug. When fulminant, this reaction can be fatal. ED is a rare disorder that may appear suddenly or gradually, occasionally accompanied by fever, chills, and lymphadenopathy. Most patients are over 40 years of age and are mostly male. Psoriasis and drug reactions are the most frequent causes of ED; it is idiopathic in up to 20% to 30% of cases.
Reported causal agents: captopril, codeine, cefoxitin, cimetidine, dapsone, gold salts, hydantoins, isoniazid, lithium, nonsteroidal anti-inflammatory drugs (NSAIDs), omeprazole, para-aminosalicylic acid, penicillins, phenylbutazone, phenothiazines, St. John’s wort, sulfonamides, sulfonylureas, thalidomide, vancomycin, and erlotinib (Tarceva).
In young children, ED is most often secondary to severe atopic dermatitis, and in infants, the most common cause is widespread seborrheic dermatitis.
Less commonly, ED has been noted as a finding in the following skin disorders:
Allergic contact dermatitis
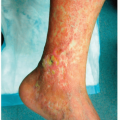
Stasis dermatitis with secondary autoeczematization
Pityriasis rubra pilaris
Graft-vs-host disease
Ichthyosiform dermatoses
Pemphigus foliaceus
Mycosis fungoides (cutaneous T ce• lymphoma)
Drug eruptions in acquired immunodeficiency syndrome (HIV/AIDS) (see Cutaneous Manifestations of HIV Disease)Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree