Fig. 1.1
Candida onychomycosis in a patient with chronic mucocutaneous candidiasis
Aside from the multiple fungal culprits, there are also multiple routes of invasion that fungi can use to infect the nail. However, in order to properly understand the different mechanisms of fungal invasion, it’s important to first have a solid grasp of nail anatomy and the process of nail growth.
The nail consists of the nail matrix, the nail plate, the underlying nail bed, and the nail folds. The nail plate is composed of hard, keratinized cells which grow out of the nail matrix – the distal, visible part of which looks like a half-moon and is called the lunula – and emerges from beneath the proximal nail fold and cuticle (which protects the nail matrix from the environment), bordered on either side by the lateral nail folds. It extends along the nail bed, and is normally cut distally, just past the hyponychium (where the skin of the fingertip meets the nail bed), at the free edge of the nail (Fig. 1.2) [14, 15].
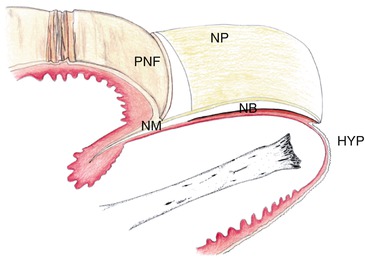
Fig. 1.2
This illustration of a sagittal section of the finger provides us with a visual of some internal and external details of nail anatomy. The nail plate (NP) grows out of the nail matrix (NM) and extends along the nail bed (NB). It is bordered proximally by the proximal nail fold (PNF) and distally by the hyponychium (HYP)
There are five generally accepted patterns of fungal nail infections, each utilizing a slightly different mechanism of invasion. They are: distal lateral subungual onychomycosis (DLSO), superficial onychomycosis (SO), proximal subungual onychomycosis (PSO), endonyx onychomycosis (EO), and total dystrophic onychomycosis (TDO) [16].
The most common form of fungal invasion of the nail is DLSO [4, 6]. This occurs when fungus invades the nail bed and undersurface of the nail plate via the hyponychium (usually as an extension of tinea pedis/manuum), and spreads proximally along the longitudinally oriented rete ridges of the nail bed.
SO was previously known as superficial white onychomycosis (SWO), but that term became too narrow once SO was found to present with other features (such as deep penetration, brown/black pigmentation, etc.) depending on the organism involved [6]. SO occurs when the fungus localizes superficially on the dorsal nail plate and forms colonies (seen as opaque, scaly plaques with distinct edges) that are easily scraped away. Some NDMs actually penetrate deeper into the nail plate, causing a deep, diffuse SO that can extend past the proximal nail fold and is visible through the cuticle [5, 17].
In PSO, the fungal elements invade the deeper, ventral aspect of the nail plate from the proximal portion of the nail and migrate distally, causing a patch or a band of leukonychia that moves distally with nail growth. PSO is a relatively uncommon subtype that can suggest the possibility of HIV infection or other types of immunosuppression [4]. It can also occur secondarily to paronychia (infection and inflammation of the nail folds) [6]. As mentioned above, when PSO is associated with periungual inflammation, we should suspect a mold infection.
EO occurs when the fungus invades the distal nail plate directly, without any involvement of the nail bed. This is a very rare presentation, characterized by nail plate invasion without subungual hyperkeratosis (because the nail bed is spared) [6, 16].
Besides those five general classifications, there are some patients that present with features from multiple forms of nail infection, called mixed pattern onychomycosis (MPO) [6, 16]. The two most common examples of this are when a nail affected with DLSO develops SO as well (especially in an area where another toe overrides it) and when SO extends under the proximal nail fold, creating an increased risk of PSO.
Eventually, if the fungal infections are allowed to progress, the entire nail will become thick and dystrophic. This end-stage nail disease is referred to as total dystrophic onychomycosis (TDO) (Fig. 1.3) [4, 6, 16].

Fig. 1.3
Total dystrophic onychomycosis. Note the severe concomitant tinea pedis
Before any of these classical presentations can occur, however, the fungus must first initiate and establish an infection. In order for it to do that, it needs to accomplish three steps: make contact, adhere to the stratum corneum, and invade the keratin layers [18]. We will examine how dermatophytes accomplish these steps.
The first phase occurs when an individual comes into contact with a contaminated surface or another affected individual. Naturally, certain areas of the body are more susceptible to infection than others, owing to anatomic and/or environmental factors such as humidity, temperature, pH, etc. Understanding this helps to explain the greatly increased frequency of toenail compared to fingernail onychomycosis (a ratio of 19:1) [19]. The warm, moist, confined environment provided by our occlusive footwear, combined with slower toenail than fingernail growth and less blood flow to the area, all combine to make the feet and toes specifically vulnerable. There are also patients with a general predisposition to contracting onychomycosis due to genetic factors [20–22].
After contact is made, the fungal arthroconidia (a primitive spore type, formed by fragmentation or disarticulation of existing hyphae) spend the next few hours (between 2 and 12) completing the second phase: adhering to the outer layer of the skin [18, 23]. Regrettably, little is known about the specific factors that mediate dermatophyte adherence [23]. We know the fungal arthroconidia produce both short and long adhesive fibrils that anchor them to the tissue surface and that the fungus secretes proteases that may modify both the surface of the epithelial cells and the fungus itself, inducing conformational changes that potentially facilitate adherence [18, 23, 24]. We also know dermatophytes express certain adhesins specific for carbohydrates present on the skin surface – but these have not been sufficiently investigated for us to determine what, if any, role they play in adherence [18, 23].
It’s important to note the resilience of the arthroconidia, as they are often the primary form involved in the spread of infection. Since they have thicker cell walls and no immediate exogenous nutritional requirements, they can persist in the environment, even under what would otherwise be hostile conditions [25, 26]. Additionally, fungal spores are greatly resistant to antifungal medication, requiring a dose 10–1000 times higher than that necessary to kill growing hyphae cells [25, 27]. This is one of the contributing factors to the high recurrence rate of onychomycosis: treatment often fails to eradicate the resistant arthroconidia, and a reservoir of infection is left behind [25, 28].
Once the dermatophytes have adhered to the stratum corneum, they release enzymes (keratinases, lipases, nonspecific proteases, etc.) which have their optimal activity at the pH level of the human skin [29]. This begins the third and final phase, by helping the germinating arthroconidia’s fungal hyphae penetrate the host tissue and scavenge for nutrients, digesting keratin into shorter peptides and amino acids to be assimilated [23, 29]. However, much of the process of fungal invasion, like the process of fungal adherence, is still not fully understood [23].
Unfortunately, the value of animal models in helping us understand dermatophyte infections is limited, as they do not perfectly mirror human infections [30]. Furthermore, most human dermatophyte infections are caused by T. rubrum, which specifically requires a human host. Animal models can still be useful, though, for evaluating diagnostic procedures and testing new treatments [30].
Outlook: Future Developments
Treating onychomycosis is problematic for a variety of reasons. Oral therapy is more effective than topical therapy, but it’s expensive, requires monitoring for toxicity, and can result in multiple drug interactions. Topical therapy is a long process that often requires nail debridement and multiple return visits and still delivers a relatively poor success rate. The very nature of the hard, protective nail plate itself makes it difficult for topical drugs to reach the fungal pathogens beneath it.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


