Frontal Sinus Cranialization
Mohamad Masoumy
Prasanth Patcha
Robert C. Dinsmore
Jack C. Yu
DEFINITION
Cranialization refers to the removal of the posterior table of the frontal sinus with occlusion of the inlet into the frontonasal ducts and allowing the neural structures, mainly frontal lobes of the brain and the intact dura, to move directly posterior to the anterior table of the frontal bone.
Cranialization is performed in patients with frontal sinus fractures when the frontonasal duct drainage is interrupted and cannot be reconstituted even with intubation or endoscopic salvage procedures.1,2,3,4
Once frontonasal duct integrity is lost, the two surgical options are cranialization and obturation. Obturation is defined as filling of the frontal sinus with grafts, often consisting of adipose tissue. Both cranialization and obturation require the complete removal of sinus mucosa and closure of the cephalic part of the frontonasal duct with two key differences.
In obturation, the posterior table must be preserved or restored. If there is any concern for CSF leak, remove the posterior table and inspect the dura for injury. During cranialization, the posterior table must be resected.
In obturation, bone, fat and other tissue are used to fill the frontal sinus space. In cranialization, this space is ultimately occupied by the brain and allows for brain edema without increased intracranial pressure; as the brain moves into this space, the anterior table of the frontal bone becomes the only bony layer of the inferior anterior cranial vault.3
ANATOMY
The frontal sinus is located in the lower 10% to 15% of the forehead and the width ranges from 2 cm to more than 10 cm. The supraorbital foramen can serve as an approximate indicator of the lateral extent of the frontal sinus. AP dimensions measure approximately 15 mm at the base with a gradual taper cephalically, extending 20 to 30 mm with a variable, scalloped border. Often a complete bony septum separates the sinus cavity into left and right compartments (FIG 1).
Mucus-secreting respiratory mucosa completely lines the internal surface of the frontal sinus. The mucous drains through a funnel-shaped outlet leading into the frontonasal duct, which opens in the infundibulum of the middle meatus of the nose.
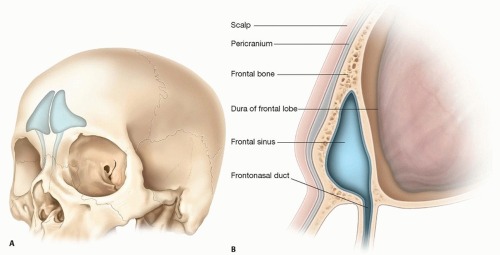
FIG 1 • A. Frontal sinuses in situ. B. Parasagittal section, normal anatomy.
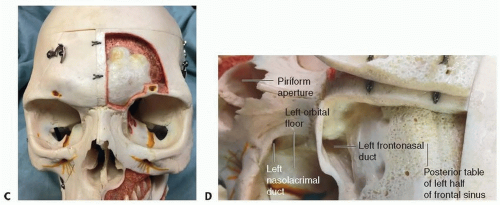
FIG 1 (Continued) • C. Supraorbital foramina (arrows) mark the lateral boundaries of the frontal sinus. The anterior table has been partially removed from the left half of the frontal sinus on this model. D. Anterior table of frontal sinus reflected.
Behind the posterior table is the triangular bony anchor of the falx cerebri, crista galli, bordered laterally by the cribriform plate of the ethmoid bone. The olfactory fibers exit the cranium into the most cephalic part of the nasal cavity to provide special visceral afferent innervations. Dural sleeves cover these olfactory fibers. In trauma, the laceration of these dural sleeves by bone fragments leads to CSF rhinorrhea.
The anterior cranial fossa directly above the nasal cavity is and must remain completely sterile. Thus, the surgeon’s primary objective in caring for patients with frontal sinus fractures is to restore this secure separation of the nose from the intracranial space to avoid infection from nasopharyngeal flora.
PATHOGENESIS
During sudden compressive loading of the forehead, as in a blunt frontal impact, the anterior table will deform rapidly. If the strain exceeds the ultimate tensile strain of the bone, it fractures. Fracturing absorbs kinetic energy and greatly reduces force transmission, protecting the frontal lobe of the brain.
Higher energy impacts can extend fractures across the apex and the floor of the sinus into the posterior table and the frontonasal duct.2
Frontal sinus trauma resulting in severe and extensive fractures of the anterior and posterior tables frequently involves the frontonasal outflow tract.
If there is greater than 25% disruption of the posterior table, cranialization should be considered.5
Another indication for cranialization is for closure after anterior skull base tumor surgeries or other craniotomy procedures involving the anterior vault.
NATURAL HISTORY
Significant frontal sinus injuries involving the posterior table or frontonasal duct can lead to the complications of mucocele, mucopyocele, osteomyelitis, late CSF leak, meningitis, and cerebral abscess. Management via cranialization during the initial fracture can help to avoid these sequelae.1,2,3,4,5,6,7,8
PATIENT HISTORY AND PHYSICAL FINDINGS
Blunt and penetrating traumas are often the cause of frontal sinus fractures. The patient may have a history of recent or remote trauma (FIG 2). In the setting of remote trauma, a high level of suspicion must be maintained for such sequelae as mucocele/mucopyocele, CSF leak (early or late), and osteomyelitis of the frontal bone.
At the time of evaluation, assess contour abnormalities of the forehead, brow, and frontonasal region. Document presenting symptoms such as paresthesia, numbness, or paralysis. Furthermore, search for associated injuries of other facial regions, the cervical spine, brain, eyes, cranial nerves, and the major neck vessels. Advance Trauma Life Support protocols should always be followed.
The initial note should document the patient’s neurological status, olfaction, visual acuity, extraocular movements, pupil size and reactivity, rhinorrhea if present, maxillary and mandibular stability, occlusion, facial movements, and sensation. Cervical tenderness is important, especially if it is out of proportion to radiological or clinical findings. Lateral neck pain could represent carotidynia, a sign of carotid artery injury.
IMAGING
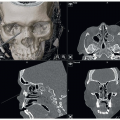
CT imaging with thin-cut axial, coronal, sagittal with 3D reconstructions is the radiologic gold standard. These images evaluate both anterior and posterior table frontal sinus fractures as well as associated intracranial, facial, and spinal injuries (FIG 3).
Some surgeons advocate intraoperative navigation using available CT data with a stable fiduciary and infrared multicamera system. The advances in stealth technology have rendered such guidance tools easier to use as well as simpler and faster to set up.
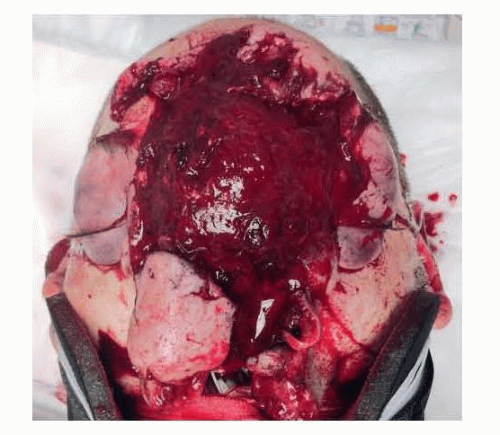 FIG 2 • Massive craniofacial wound from shotgun blast at close range. |
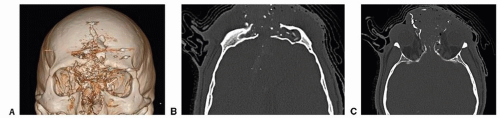 FIG 3 • A. 3D CT reconstruction demonstrating comminuted facial fractures with concomitant frontal sinus injury from the shotgun blast. B. Axial CT demonstrating massive injuries to the anterior and posterior tables of the frontal sinus with segmental bone loss. C. Axial CT image showing destruction of the frontonasal duct. |
DIFFERENTIAL DIAGNOSIS
Frontal sinus fractures need to be further characterized using the following variables to best guide treatment:
Extent of injury to the anterior and posterior tables including severity of displacement and comminution
The status of the frontonasal duct
Dura integrity
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree