CHAPTER 10 Foundation facelift
History
Foundation facelift, formerly known as deep-plane lift, is characterized by elevation of a composite musculo-cutaneous flap of facial and upper cervical soft tissues. As the flap is rotated to a more lateral and cephalad position, it dramatically corrects tissue laxity, and rejuvenates the face. The foundation facelift is particularly effective in softening the nasolabial fold. The thickness and excellent vascularity of the flap produce long-lasting and natural results.
Patient evaluation
Foundation facelift is particularly useful in certain classes of patients.
• Patients who have had a previous SMAS-platysma operation and in whom the remaining SMAS-platysma may be insubstantial and/or scarred can still have a robust flap when the subcutaneous tissues and skin remain integrated with the SMAS-platysma as in the foundation facelift.
• Because the foundation facelift flap has a particularly strong blood supply, typical of musculo-cutaneous flaps, this operation is a good choice for smokers and other patients in whom the vascularity of the facelift flap may be suboptimal.
• The dissection plane deep to the SMAS-platysma is an avascular plane, and operations in this plane are bloodless, rarely eventuating in hematomas. The foundation lift, then, is a good choice for patients at increased risk for postoperative bleeding.
• Because the foundation facelift flap is thick and has a robust blood supply, it can be elevated to the nasolabial fold and even on to the lip without fear of flap necrosis, even when the flap is pulled up under some tension. This operation, is a champion technique for flattening deep nasolabial folds.
• Evaluate the skin of the face and neck and underlying soft tissues for laxity and loss of elasticity. Laxity is characterized by excess and redundant skin. Loss of elasticity means that the skin does not easily snap back after being put under stretch, and mitigates against a superior and long-lasting result. These patients should be warned that an early secondary operation may be necessary.
• Severe sun damage, as evidenced by rhytids, thinning of the skin, and pigmentary changes, should also be noted and pointed out to the patient. These actinic changes are little improved by facelifting, and the patient should be aware of the limitations imposed by solar damage to the skin.
• Ptosis of the platysma, evidenced by vertical bands in the anterior neck, will almost always require anterior platysma plication for correction.
• Note presence of excess fat in the neck, as removal of this excess is a sine qua non for creating a youthful neck and jaw line.
• Jowling and deep nasolabial folds should be noted. These hallmarks of facial aging are well-treated with foundation facelift.
• Descent of the malar fat pad is also a cardinal sign of aging. Its correction requires movement of the fat pad and skin in a vertical, cephalic direction.
• The quality and thickness of the preauricular skin and the presence of fine hairs on the skin should be noted in women and men. Thick, hair-bearing skin in either sex is a relative contraindication to using a retrotragal incision, since transposing the thickened, hair-bearing skin to cover the tragus will obscure the fine detail of this important anatomic landmark.
Anatomy
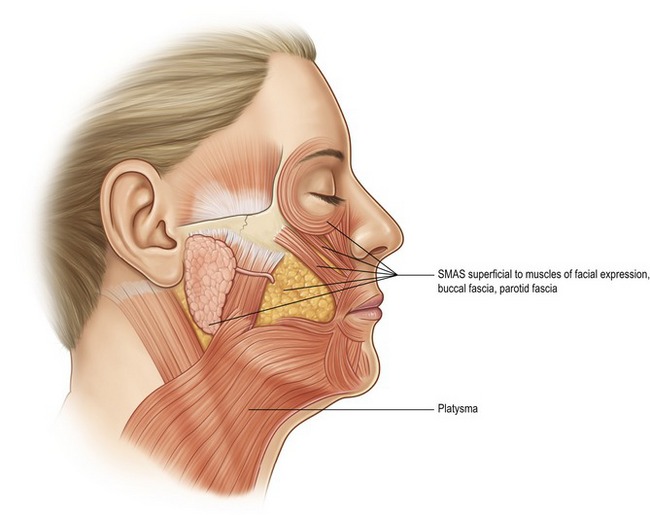
From its origin in the lower neck, the platysma muscle extends to the lower cheek, covering a portion of the lower parotid gland before inserting into the perioral muscles at the corner of the mouth (Fig. 10.1). The investing fascia of the platysma continues cephalad in the cheek as the SMAS (superficial musculo-aponeurotic system). The SMAS lies superficial to the masseter muscle and the buccal fat pad, before continuing in a cephalic direction to invest the deep and superficial layers of the zygomatic major and minor.
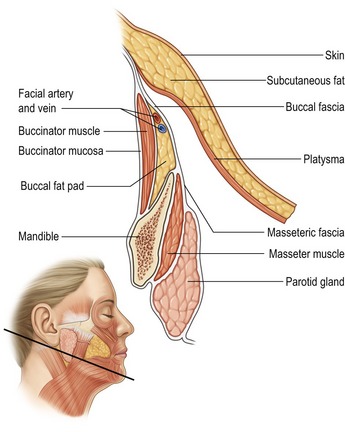
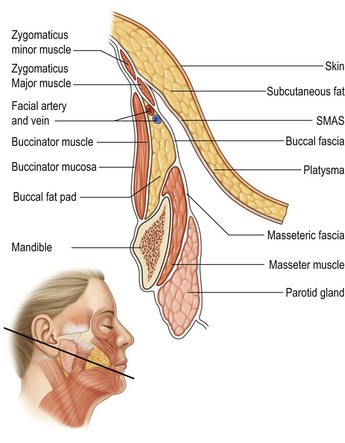
The defining feature of the foundation facelift is elevation of the SMAS-platysma, subcutaneous fat, and overlying skin as a unified flap. The SMAS-platysma is the integrated foundation of this musculo-cutaneous, composite flap. In the upper neck and lower cheek, the platysma is the deepest layer of the flap (Fig. 10.2); in the mid and upper cheek, the platysma continues as the SMAS and forms the deepest layer of the flap (Fig. 10.3).
As the nerve branches exit the parotid gland, they lie deep to two important fascial planes:
• The more superficial and thicker plane is the SMAS-platysma.
• Just deep to the SMAS-platysma is a thin layer of fascia lying just superficial to the nerve branches.
• As the zygomatic and buccal branches course in a cephalad direction, they are covered by the zygomaticus major and minor muscles (Figs 10.3 and 10.4).
• A more complete understanding of the anatomy of the foundation facelift is obtained by studying an artist’s representation of the surgeon’s view when the flap is elevated (Fig. 10.5). The platysma is elevated with the subcutaneous fat and skin in the lower cheek. In the mid and upper cheek, the platysma becomes the SMAS and is also elevated with the subcutaneous fat and skin. The malar fat pad in the upper cheek also remains attached to the skin and is elevated as the skin is mobilized and repositioned. Note the course of the branches of the facial nerve as they exit the anterior border of the parotid gland, but remain covered by masseteric fascia, buccal fascia, and the zygomaticus major.
Technical steps
Marking the patient
Prior to surgery, anatomic landmarks are drawn on the face and neck with the patient standing (Fig. 10.6). The drawn lines indicate:









