Fig. 19.1
Distribution of breast reconstruction procedures by type. Courtesy of the American Society of Plastic Surgeons 2014 (DTI direct-to-implant, TE tissue expander, TRAM transverse rectus abdominis muscle, DIEP deep inferior epigastric perforator)
As our understanding of patient selection has improved, there are greater opportunities for the plastic surgeon to offer direct-to-implant (DTI) reconstruction provided the vascularity of the skin flaps can be accurately assessed intraoperatively. Today approximately 15–20 % of women undergoing implant-based reconstruction receive a direct-to-implant operation [14]. DTI reconstruction allows for a one-stage reconstruction potentially avoiding the need for a second operation. DTI reconstruction has been shown to reduce cost and number of office visits, eliminate the need for uncomfortable tissue expanders, expedite time to radiation, and offers patients immediate aesthetic results [14, 17–20]. This single-stage procedure is also psychologically superior to two-stage reconstruction [21]. This offers an ideal reconstructive choice in select patients by recreating the breast at the time of mastectomy with a single operation. This technique has been attempted—and abandoned—in the past due to its technically demanding nature, issues with pectoralis muscle retraction, implant malposition, capsular contracture, and concern for implant exposure in thin-skinned individuals. These concerns have largely been obviated with the introduction of ADM. Using ADM for inferior and lateral pole coverage affords the surgeon the ability to maintain the pectoralis position, reliably delineate implant position in a single stage, and lower the risk of capsular contracture by inhibiting the foreign-body tissue response [14, 22, 23]. Furthermore, DTI reconstruction with human ADM has been shown to be a cost-efficient option, with a total cost less than that of traditional staged reconstruction without ADM [24]. Despite this, the inability to accurately assess skin flap viability immediately following the mastectomy raised concern over mastectomy skin flap or NAC necrosis limiting DTI reconstruction to carefully selected patients, specifically those with small breasts preoperatively and/or appreciably thick mastectomy skin flaps.
Overall concern for poor mastectomy flap perfusion can be addressed with the use of intraoperative indocyanine green (ICG) angiography (SPY Elite, Novadaq Technologies Inc., Mississauga, ON). The SPY Elite imaging system allows real-time, intraoperative clinical assessment of skin flap viability with a technology that provides qualitative and quantitative interpretation of skin flap perfusion.
The History of Fluorescence Imaging
Indocyanine Green (ICG) first saw its introduction to medicine during the 1950s. An executive from Eastman Kodak began helping Dr. Irwin Fox from the Mayo Clinic develop a dye biocompatible with blood. ICG exhibits a high affinity for serum albumin (98 %) and absorption near infrared (NIR) at 805 nm. Approved by the FDA in 1956, the Baltimore pharmaceutical firm Hynson, Wescott, & Dunning turned ICG from a substance unstable in aqueous solution to the lyophilized form used today. Shortly thereafter, ICG saw its first use for medical research in cardiology, measuring time varying dilution in whole blood as a way to evaluate cardiac output in valvular and septal defects [25]. The first attempts at using ICG for angiography was by Kogure and Choromokos in 1969 when they demonstrated infrared absorption angiography in the canine brain vasculature [26]. These efforts were further refined by Hochheimer [27] and Flower [28], who demonstrated the potential use of ICG in the aging and glaucomatous human eye [29, 30].
While ICG has been used for several decades in retinal angiography, fluorescein has been much more popular partly because it is visible without camera equipment [31]. Fluorescein remained the gold standard for evaluating superficial vascular structures in the fundus, identifying perfusion permeability, and proliferative abnormalities [29]. Nonetheless, ICG gives information of deeper lying blood vessels due to its NIR wavelength in which tissues are more translucent than in visual wavelengths without tissue chromophores interfering. Additionally, ICG does not stain tissues like fluorescein allowing multiple repeated images to be obtained in the same operative session.
The concept of fluorescence involves illuminating the tissue of interest with a light at the excitation (strong) wavelength (750–810 nm) while observing the fluorescing (weak) rays in the sensor (over 800 nm). Camera, filters, and a light source are required to prevent mixing of excitation and fluorescing rays to detecting sensors. Clinical value was initially hampered by the lack of photographic resolution and primitive technology to record the data. The introduction of digital angiography with highly weighted cameras in the NIR wavelength, partnered with high speed imaging provided clinicians with the ability to translate data into clinical use [32].
In 2005, the FDA approved the ICG angiography SPY for coronary angiography. Indocyanine green can be either used to evaluate myocardial tissue perfusion by imaging an area of interest around a coronary vessel or direct imaging of the graft by visualizing the lumen. Noncardiac surgeons soon saw the utility in a device that provided real time information regarding tissue perfusion. Shortly thereafter, SPY Elite received FDA clearance for use in plastic surgery, organ transplant, and gastrointestinal surgical procedures.
Indocyanine Green
ICG’s advantages are its high affinity towards plasma proteins, specifically albumin, leading to confinement within the vascular space, low toxicity, short half-life in circulation, and rapid excretion, almost exclusively by the liver into bile. ICG has an excellent safety profile with a low incidence of adverse events [33]. Sodium iodide composes no more than 5 % of most ICG formulations, making the only true contraindication to its use patients with severe iodine and shellfish allergies.
After injection, ICG is bound within a few seconds to lipoprotein complexes and remains intravascular, with normal vascular permeability [34]. Exact wavelength of ICG excitation and fluorescence depends on the chemical environment and physical conditions, such as temperature and concentration [31]. Binding to blood proteins shifts the excitation peak from 780 to ~805 nm and the fluorescence peak to ~835 nm in several minutes.
With a half-life of 2.5–3 minutes, ICG is excreted exclusively by the liver via glutathione S-transferase without modification or reabsorption from the intestine [31]. There is negligible renal, lung, peripheral, or cerebrospinal uptake of dye [35]. This allows repeated administration within the same surgical procedure, in comparison with fluorescein which remains within the tissue for 12 h.
SPY Elite Imaging
The SPY Elite system is comprised of a near-infrared light source, a maneuverable imaging head and a digital camera. In the operating room, the articulating arm which contains the camera is positioned over the patient. ICG is then injected through a peripheral line by the anesthetist. As the ICG binds with albumin within vascularized tissue, a blush appears on the screen. Video of the procedure can be captured and quantification software is available to look at relative perfusion values. A digital display is present on two opposing screens allowing visualization by both the device operator and the surgeon (Fig. 19.2).
Fig. 19.2
SPY Elite imaging syste m
The maximum field that can be illuminated by the laser optical system is approximately 18.5 × 13.5 cm2. The cameras can capture images at 3.75–30 frames per second, with a recording time between 30 and 120 s. Coupled software (SPY-Q Analysis Toolkit) provides additional views, comparisons, analysis tools, including fluorescence intensity measurement algorithms. Gurtner et al. 2013 published technical recommendations of use of SPY in plastic surgery with guidelines on timing of evaluation [36].
Fluorescence Imaging in Breast Reconstructio n
Since its introduction in 2007, intraoperative indocyanine green angiography using the SPY Elite system has been shown to be a reliable method for evaluating mastectomy skin flap and tissue flap perfusion [37]. A prospective trial evaluating its use in post-mastectomy breast reconstruction has demonstrated that it possesses a 90 % sensitivity for detection of tissue necrosis [38]. Furthermore, comparative cost studies have established that appropriate use of the SPY Elite system reduces the incidence of reoperation for ischemic complications, thereby reducing healthcare related expenditure in prosthetic based breast reconstruction [37, 39, 40]. Moreover, the use of SPY Elite has also been shown to theoretically reduce the risk of capsular contracture, by selecting for only well-perfused skin flaps which are better able to combat sub-clinical infection [37].
In autologous tissue breast reconstruction using the deep inferior epigastric artery perforator (DIEP) flap or the transverse rectus abdominis (TRAM) flap, ICG angiography has proven its utility in identifying areas of poor flap perfusion and enhancing our understanding of flap microvasculature [41–43]. Notably, evidence from several studies have shown that the SPY Elite system is superior to clinical judgment alone in predicting areas of future flap necrosis [42, 43]. Moreover, its use has also been shown to produce a cost-savings benefit by reducing the need for reoperation due to flap necrosis or flap congestion [44]. Although it can only provide information a few millimeters deep from the skin, one of the most significant advantages of ICG angiography is its ability to calculate intrinsic transit time through the vascular anastomosis and thereby provide real-time information regarding the risk for venous congestion [42, 45]. The main limitation of ICG angiography in microsurgical breast reconstruction is its inability to predict perforator location based on signal intensity readings [43]. Indeed, the functions of CT angiography and ICG angiography in autologous breast reconstruction planning are in contradistinction; whereas CT angiography has been shown to accurately assess size and location on perforating vessels, ICG angiography is able to evaluate the actual perforasome of a given vessel [45, 46]. Nevertheless, as understanding of DIEP flap vascular anatomy has improved, surgeons have recognized that perforators tend to arise in predictable locations, and the use of imaging (CT angiography) to identify perforator location is increasingly being abandoned. What has been found to be of greater importance is an understanding of DIEP/TRAM flap microsurgical perfusion patterns. Partly through the use of ICG angiography, these patterns have been clearly elucidated in the last decade [41, 47, 48].
Rapid and reliable DIEP flap harvest can be accomplished by attempting lateral dissection first in order to identify a lateral row perforator. When this fails, direction should then be turned to the periumbilical region, where perforators commonly originate within 5 cm of the umbilicus. Lastly, medial row perforator harvest should be attempted. It is now understood that lateral row perforators are better able to perfuse the hemiabdomen and follow the perfusion pattern described by Holm et al., in which Zones I and II compromise the entire hemiabdomen [41, 48, 49]. This is in contrast to the pioneering work of Hartrampf in which Zone II compromised the medial portion of the contralateral hemiabdomen [50]. This classic pattern of perfusion, however, is followed by medial-row DIEP perforators [48, 49]. This understanding of microvascular perfusion is further enhanced by intraoperative ICG angiography, which is able to detect areas of ischemia in the lateral and inferior aspects of the flap with high sensitivity. Lastly, the SPY Elite system affords the ability to evaluate dominance of the superficial or deep system for selection of appropriate vessel anastomosis [51].
At our institution the SPY Elite system is a vital adjunct to clinical decision-making when performing prosthetic or autologous breast reconstruction. Its merits include assessment of the NAC in nipple-sparing mastectomy, ability to determine feasibility of DTI reconstruction, predicting areas of mastectomy flap ischemia or congestion, and evaluation of arterial inflow and venous outflow in autologous tissue reconstruction.
Nipple-Sparing Mastectomy with Partial Subpectoral Direct-to-Implant Breast Reconstruction and Acellular Dermal Matrix (ADM)
Nipple-sparing mastectomy (NSM) with immediate direct-to-implant breast reconstruction represents the pinnacle of reconstructive surgery through which natural form, symmetry, and the feminine aesthetic can be immediately offered to the patient at the time of oncologic surgery. Preoperatively patients are extensively counseled regarding reconstructive options. Included in the preoperative consult is the fact that ICG angiography will be performed to assess skin flap viability for direct-to-implant reconstruction. Patients are counseled and informed that if there is questionable perfusion of mastectomy skin flaps, DTI reconstruction may be abandoned and a tissue expander will be placed at the discretion of the plastic surgeon. A specific advantage of the imaging system is the feature that allows printing of the SPY images in the operating room. This provides a hard copy of the images that can be included in the medical record and shared with the patient postoperatively, allowing them insight into the surgeon’s intraoperative decision making.
At our institution, the majority of nipple-sparing mastectomies are performed via an inframammary fold (IMF) incision by the oncologic breast surgeons. This maintains NAC viability, allows for discrete scar placement, and minimizes nipple malposition postoperatively compared to peri-areolar or radial incisions. The SPY Elite system is used to interrogate the mastectomy skin flaps in order to assess skin flap viability before and after implant insertion. Although 10 cc of ICG are included in the SPY PAQ kit (along with a sterile drape and an aqueous solvent), only 3 cc need be used at once. This allows a total of three possible interrogations of the mastectomy skin flaps with a single kit.
There are times when the breast surgeons at our institution perform tumescent technique when performing mastectomy for hemostasis and assistance in dissection of mastectomy planes [52]. Tumescent has been previously shown to cause hypoperfusion voiding ICG readings [53]. We have confirmed this in our own practices anecdotally. Initially, we tested spy with 1 ampule (1 mg) of epinephrine in a 1 liter normal saline bag. We then decreased the doses to 0.7, 0.5, and 0.3 mg. While 0.3 mg does not seem to affect ICG readings significantly, the breast surgeons have noted it does not provide the desired hemostatic effect. We avoid direct-to-implant reconstruction and default to expander placement in cases where tumescence has been used, due to the unpredictability of mastectomy flap perfusion both clinically and with the SPY. At this time we are actively working on a technique where tumescent solution and SPY can be used in harmony.
Surgical Techniqu e
At the completion of the nipple-sparing mastectomy, the patient is re-prepped with betadine and re-draped. The SPY Elite system is positioned next to the patient and draped with a sterile drape. Any packing is removed from the breast pocket and the skin flaps are returned to a tension free position. The articulating arm allows placement of the camera over the operative field. The operating room lights are turned off, and the mastectomy skin flaps are then interrogated using 3 cc of ICG with a 10 cc normal saline flush given by the anesthesia team. If there are no areas of poor-perfusion, the decision is made to proceed with DTI reconstruction (Fig. 19.3).
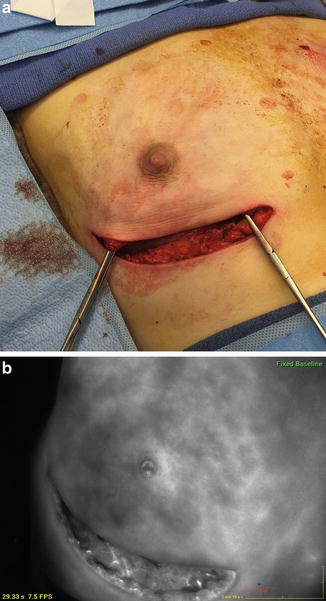
Fig. 19.3
(a) Clinical image of mastectomy flap immediately following NSM. (b) Corresponding SPY Image showing good tissue perfusion throughout the flap and NAC
When performing a subpectoral reconstruction , a pocket is created beneath the pectoralis major muscle which covers the superior third of the implant. The pectoralis is raised from lateral to medial to the level of the clavicle, and is released from its origin along the sternal border for the inferior 2–3 cm. Next, ADM is opened and prepared. The ADM is then sutured to the inferior border of the pectoralis with a 3-0 Vicryl suture in a continuous running fashion. A degree of pleating is allowed while securing the ADM to the pectoralis medially in order to allow for medial pole fullness. The medial third of the ADM is then secured to the chest wall and IMF using 3-0 Vicryl simple interrupted sutures.
In the situation where the vascularity of the flaps is in question, we proceed with the reconstruction: release of the pectoralis from its origin and sew the ADM to the caudal border of the pectoralis, followed by placement of a temporary sizer. In our experience, a marginal SPY image immediately at the end of the mastectomy may be due to over retraction of the skin flaps during the extirpative surgery. The SPY is then repeated with the sizer in place. In the situation where the SPY continues to appear marginal or nonfavorable (Fig. 19.4), the reconstruction is converted to a tissue-expander reconstruction with low or no intraoperative filling and closed primarily.
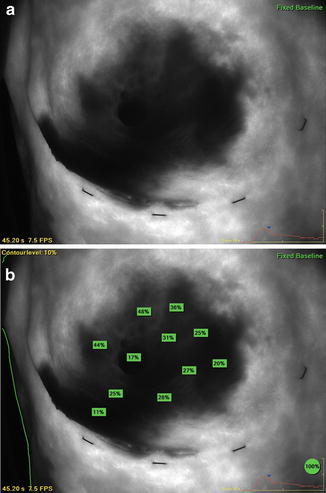
Fig. 19.4
(a) SPY Image showing poor perfusion of the mastectomy flap immediately following NSM. (b) Quantitative relative values indicating poor tissue perfusion. Note that the 100 % reference marker is placed over the sternum. In this case, DTI reconstruction was aborted and a tissue-expander was placed
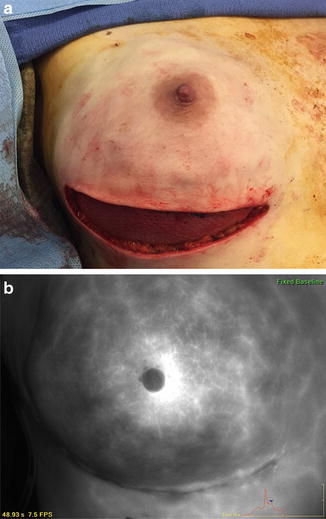
Provided that the SPY images show well-perfused flaps, the implant is removed from its packaging and allowed to soak in a triple antibiotic solution in its container (1 g cefazolin, 80 mg gentamicin, and 50,000 IU bacitracin). The breast pocket is then copiously irrigated with triple antibiotic solution as well. Surgeon’s gloves are changed and the implant is inserted beneath the pectoralis/ADM construct using a one-touch technique. The inferior aspect of the ADM is next secured to the IMF using 3-0 Vicryl simple interrupted sutures, and laterally is secured to the chest wall just posterior to the lateral border of the implant in order to medialize the prosthesis and prevent lateral migration. A #7 Jackson-Pratt drain is next introduced through a lateral stab incision, and inserted between the ADM and the mastectomy flap.
The mastectomy skin flap incisions are tailor-tacked using staples, and re-interrogated using the SPY Elite system (Fig. 19.5). Relative perfusion values can be obtained by placing a reference marker on tissue that is known to be well-perfused (we prefer an area over the sternum). Quantitative relative values are useful, not only to assess tissue perfusion, but also to assess for flap congestion caused by undue tension on the overlying flap by the implant. Any areas of ischemic perfusion at the incision site are excised at this time and the patient is closed primarily using 3-0 Monocryl deep dermal sutures, and a 3-0 Monocryl subcuticular pull-through suture. DermaBond (Ethicon, Somerville, NJ) is applied to the incision site in order to provide an occlusive seal and prevent bacterial entry into the wound. The drain is secured using a 3-0 Nylon suture, a BioPatch (Ethicon, Somerville, NJ) is placed in order to prevent bacterial migration through the drain-site, and the drain site is covered with a transparent film dressing. Finally, the patient is placed in a surgical bra prior to transfer to the surgical bed (Fig. 19.6).
 Patient Selection and Breast Imaging
Patient Selection and Breast Imaging
 Plastic Surgery Considerations in Reconstruction After Nipple-Sparing Mastectomy
Plastic Surgery Considerations in Reconstruction After Nipple-Sparing Mastectomy
 Nipple and Breast Anatomy
Nipple and Breast Anatomy
 The Inframammary Approach to Nipple-Sparing Mastectomy: The Georgetown University Hospital Experience
The Inframammary Approach to Nipple-Sparing Mastectomy: The Georgetown University Hospital Experience
 Management of Complications Following Nipple-Sparing Mastectomy
Management of Complications Following Nipple-Sparing Mastectomy
 Techniques to Avoid Nipple and Flap Necrosis
Techniques to Avoid Nipple and Flap Necrosis




Related posts:
Patient Selection and Breast Imaging
Plastic Surgery Considerations in Reconstruction After Nipple-Sparing Mastectomy
Nipple and Breast Anatomy
The Inframammary Approach to Nipple-Sparing Mastectomy: The Georgetown University Hospital Experience
Management of Complications Following Nipple-Sparing Mastectomy
Techniques to Avoid Nipple and Flap Necrosis
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
