Femoral and Adductor Canal Blocks
Sarah Madison
Jean-Louis Horn
DEFINITION
A peripheral nerve block is an analgesic technique in which local anesthetics are injected percutaneously in proximity to a sensory nerve.
The location of the injection determines the distribution of analgesia.
Femoral nerve block may be used for postoperative analgesia for procedures on the anterior thigh, knee, medial leg, or medial ankle.
Adductor canal block may be used for postoperative analgesia for procedures on the knee or medial leg.
A continuous infusion of local anesthetic via a perineural catheter can provide analgesia for several days after surgery.
Nerve blocks are often part of a multimodal regimen that also includes systemic medications.
Nerve blocks can reduce pain and opioid consumption and enhance satisfaction and recovery.1
Depending on the location and extent of surgery, nerve blocks may be used for surgical anesthesia.
ANATOMY
The femoral nerve arises from the lumbar plexus and is formed by the ventral rami of L2-L4.
In the area of the femoral triangle, the femoral nerve lies deep to the fascia iliaca, lateral to the femoral artery, and superficial to the iliacus muscle.
The femoral nerve divides into anterior and posterior divisions and descends as the saphenous nerve to the medial leg.
The posterior branch provides motor innervation to the quadriceps muscles as well as sensory articular branches to the knee joint.
The saphenous nerve, obturator nerve (posterior division), and the nerve to the vastus medialis lie within the adductor canal.
The adductor canal is bounded by the sartorius and the vastoadductor membrane medially, the vastus medialis anteriorly, and adductor longus and magnus muscles posteriorly.
The adductor canal also contains the femoral artery and vein.
The saphenous nerve and the nerve to the vastus medialis supply sensory branches to the knee.2
PATIENT HISTORY AND PHYSICAL FINDINGS
A preoperative history and physical must be performed prior to any anesthetic technique.
A thorough history and physical exam will include anesthetic history, exercise tolerance, cardiopulmonary examination, and airway examination.
Any pre-existing neuropathies in the distribution of the block should be defined and documented.
Any local infections, masses, previous surgeries, or other irregularities at the site of injection should be identified.
IMAGING
Ultrasound imaging confers efficiency and increases the success rate of most peripheral nerve blocks.
Using a high-frequency linear transducer, scan in a transverse orientation at the level of the inguinal crease. The femoral artery and femoral nerve should be easily identified in cross-section (FIG 1).
The adductor canal block is often performed in a location that is proximal to the true adductor canal, near the point at which the sartorius muscle covers the femoral vessels. The nerve can be visualized next to the femoral artery, just deep to the sartorius muscle (FIG 2).
NONOPERATIVE MANAGEMENT
The balance of risks and benefits must be considered before any nerve block. Sometimes, it is more appropriate to only employ systemic medications for pain control.
Opioids and nonopioid adjuvant medications may be used when medically appropriate, with or without a nerve block.
SURGICAL MANAGEMENT
Femoral nerve block is indicated for postoperative analgesia of the anterior thigh, knee, medial leg, or medial ankle, or for surgical anesthesia of the anterior thigh.
When combined with a sciatic block, it can be used for surgical anesthesia of the foot/ankle.
Local anesthetics will affect both motor and sensory nerves. Blocking the femoral nerve at the level of the inguinal crease results in quadriceps weakness.
Adductor canal block is indicated for postoperative analgesia of the knee, medial leg, or medial ankle.
It can be used as a surgical anesthetic in conjunction with a sciatic block for procedures on the foot/ankle.
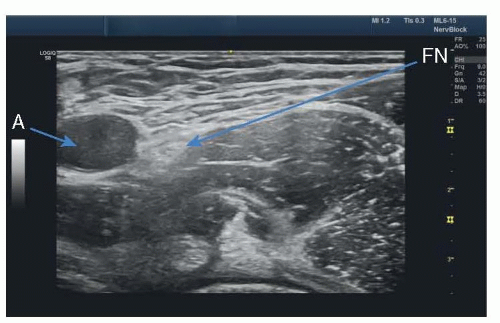
FIG 1 • Ultrasound image of femoral nerve block. FN, femoral nerve; A, femoral artery.
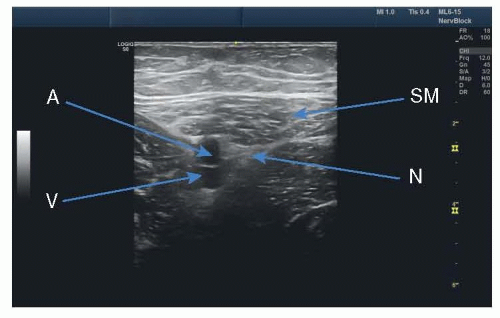
FIG 2 • Ultrasound image of adductor canal block. SN, saphenous nerve; SM, sartorius muscle; A, femoral artery; V, femoral vein.
A nerve block in the adductor canal is less likely to cause quadriceps weakness than a femoral nerve block; however, local anesthetic may spread proximally and affect motor nerves.
The nerve to the vastus medialis is reliably anesthetized with an adductor canal block, but the overall effect on quadriceps function is minimal.3
Preoperative Planning
Surgical site, extent of incision, anticipated degree of pain, and any pre-existing conditions that increase risk of complications should be considered before offering the patient a nerve block.
Postoperative ambulatory status should be determined to optimize dosing.
Crutch training, if appropriate, should take place prior to surgery.
Inpatients should be labeled as a “fall risk” and should not get out of bed without assistance.
Femoral nerve blocks for outpatients should be carefully considered and only performed with close follow-up and an otherwise low risk of falls.
The use of crutches and a knee immobilizer may attenuate fall risk with ambulation after a femoral nerve block.
Positioning
The patient should be positioned supine with the operative leg slightly externally rotated.
The bed should be flat with hips extended.
The patient’s ipsilateral hand may be kept out of the sterile field by lightly taping it to the chest.
The operator should stand on the side to be blocked, with the ultrasound machine on the other side of the patient.
Approach
With the use of ultrasound, the nerve may be approached either in-plane (needle parallel to transducer surface) or out-of-plane (needle perpendicular to transducer surface) with the ultrasound probe placed in a transverse orientation.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree