Key Words
fat grafting, breast reconstruction, implant reconstruction, autologous reconstruction, contour abnormalities
Introduction
Autologous fat grafting to the breast is a widely used and accepted adjunct in breast reconstruction today. The technique involves harvest of fat from patient-specific donor sites, fat processing, and subsequent transfer in order to improve depressions and step-offs, which may exist at the junction of the reconstructed breast and chest wall, or following lumpectomy.
First introduced in 1895 by Czerny, fat grafting was utilized when an excised lipoma was transferred to the breast to reconstruct a breast defect. In the early 20 th century, fat grafting gained momentum, however the practice of fat grafting did not become popular until the 1980s. In 1987, however, the American Society of Plastic Surgeons (ASPS) banned autologous fat grafting of breasts over concern for future cancer surveillance in the setting of fat necrosis. In 2007, the ASPS established a task force to re-evaluate the potential hazards of fat grafting, and concluded that radiographic technology could distinguish grafted fat from potentially dangerous lesions. Therefore, the ASPS Fat Graft Task Force lifted the ban on fat grafting in 2009 when it determined from a limited number of studies that there appeared to be no interference with breast cancer detection.
Numerous recent studies have demonstrated the regenerative capabilities of transferred fat, including improved angiogenesis, dermal thickness and elasticity, and radiation-induced fibrotic changes. For this reason, fat grafting has become a useful adjunct and workhorse in lumpectomy defects as well as autologous and implant-based breast reconstruction, particularly in radiated fields.
Successful fat grafting requires close attention to the recipient site compliance and capacity, as well as thorough fat harvesting, processing, and delivery technique. Here, we discuss the current indications for autologous fat grafting as an adjunct in breast reconstruction and review pertinent aspects of the preoperative patient evaluation. We describe operative techniques including donor-site selection, fat harvesting and processing. We conclude with several case examples and a review of postoperative complications and their management.
Indications and Contraindications
Autologous fat grafting is indicated for the correction of contour deformities and step-offs following autologous or implant-based post-mastectomy breast reconstruction, which often occur at the periphery of the breast reconstruction. Transferred fat may also be utilized to improve the contour of lumpectomy defects. However, established and safe indications for autologous fat grafting vary by breast reconstruction modality.
Implant-Based Reconstruction
In implant-based reconstruction, thin mastectomy flaps may lead to visible implant borders or implant rippling. Fat grafting may be utilized in these cases to camouflage implant rippling or smoothen the transition superiorly between the native chest wall and the implant. Fat grafting is commonly first performed at the time of tissue expander-to-implant exchange. However, in cases of direct implant reconstruction, fat grafting is often performed as a secondary procedure. It should be noted that patients may require several fat-grafting procedures in order to achieve desired results.
Autologous Reconstruction
In autologous reconstruction, fat can be used to smoothen the transition (or “step-off”) between the flap and chest wall. Additionally, fat grafting has been described to augment the overall volume of smaller flaps or failed flaps. While fat grafting is more frequently performed approximately 3–6 months following flap transfer, some surgeons opt to fat graft potential flaps prior to free tissue transfer.
Lumpectomy Defects
Fat grafting is a useful adjunct in the correction of contour abnormalities and breast asymmetry following lumpectomy. In the case of breast conservation therapy, a lumpectomy (or partial mastectomy) may be performed with adjuvant radiation therapy, where up to 30% of patients report dissatisfaction with aesthetic results. While radiated lumpectomy defects can represent a hostile environment, transferred fat has been shown to improve breast contour, as well as skin and soft tissue quality following radiation therapy thereby improving aesthetic outcomes. Again, patients may require more than one fat-grafting procedure in order to achieve desired results.
The only absolute contraindication to autologous fat grafting in breast reconstruction is lack of donor-site availability, which may be seen in an underweight patient. Additionally, patients with medical co-morbidities placing them at operative risk should not be offered fat grafting ( Box 20.1 ).
Established Indications
Implant-Based Reconstruction
- •
Mastectomy skin flap irregularities
- •
Step-off at implant border
- •
Implant rippling
Autologous Reconstruction
- •
Step-off at flap border
- •
Depression from fat necrosis
- •
Augmentation of flap volume
- •
Radiation fibrosis
Established Contraindications
- •
Lack of donor site availability
- •
Serious medical comorbidities
Preoperative Evaluation
A thorough history and physical exam is obtained from the patient. History should include medical co-morbidities and oncologic history, including prior surgery or radiation treatment. Physical exam involves analysis of the defect and preoperative patient photographs. Additionally, three-dimensional imaging is a useful tool in helping the surgeon determine the amount of fat to be grafted. In cases of unilateral reconstruction, the contralateral breast can be used as a reference point.
The physical exam should also include evaluation of potential donor sites, primarily the abdomen, flanks, saddlebag region, and medial thighs. The site selected is based on both patient preference and ease of harvest.
The risks and benefits of fat grafting should be discussed with the patient and informed consent obtained. Risks include but are not limited to bleeding, seroma, infection, scarring at access incisions, continued contour abnormalities, fat resorption, and need for implant replacement or future operation.
Surgical Techniques
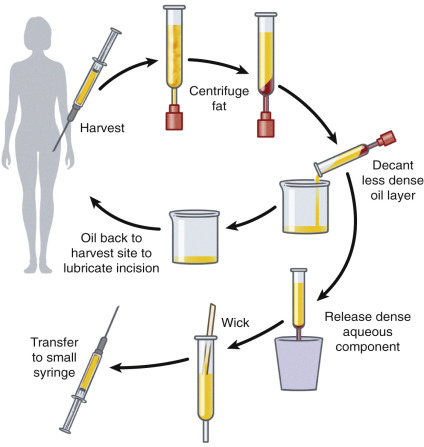
The three critical steps of autologous fat grafting are fat harvest, processing, and grafting. There are various techniques for each step, all with the aim of preventing adipocyte trauma and maximizing cell viability ( Fig. 20.1 ).
Timing
A well-vascularized recipient bed is critical in maximizing adipocyte viability. Optimization of recipient conditions includes waiting 3 months following prior breast surgery in order to minimize edema and allow for better demarcation of the contour defect, as well as allow for revascularization. Similarly, patients are often instructed to wait 6 months in between fat-grafting procedures to allow for resolution of edema and adequate wound bed revascularization.
Donor-Site Selection
The location of fat deposits in the body varies between patients. The plastic surgeon should carefully evaluate the patient and have a conversation with the patient regarding possible donor sites. As mentioned previously, these potential donor sites include the abdomen, flanks, trochanteric or “saddlebags” region, and medial thighs.
Fat Harvesting
Prior to harvesting of fat, the proposed area for harvest is infiltrated with tumescence containing lidocaine and epinephrine diluted in lactated Ringer’s or normal saline. Tumescence serves to hydrodissect the tissue planes and increases the volume of the target fat layer, thereby facilitating fat harvest. It additionally helps to decrease postoperative pain and ecchymosis.
Currently, the most commonly utilized techniques for fat harvesting include vacuum aspiration and syringe aspiration. High vacuum pressures of conventional liposuction and power-assisted liposuction may disrupt adipocyte cell structure. Instead, maintaining low negative-pressure lipoaspiration is preferred and may yield fat faster than syringe aspiration, especially useful when a large volume of fat is needed.
Additionally, cannula size may affect the viability of harvested fat. Large-bore cannulas may reduce the incidence of cell rupture and better preserve tissue architecture. In the Coleman technique for fat harvesting, a 3-mm blunt-edged 2-hole cannula is connected to a 10-mL syringe and fat is suctioned manually by withdrawing the plunger to create gentle negative pressure.
Fat Processing
Fat processing is necessary because the lipoaspirate contains not only adipocytes but also collagen fibers, blood, and extracellular debris, which can incite an inflammatory response. The various described fat processing techniques include gravity separation, centrifugation, and Telfa processing (Covidien, Minneapolis, MN).
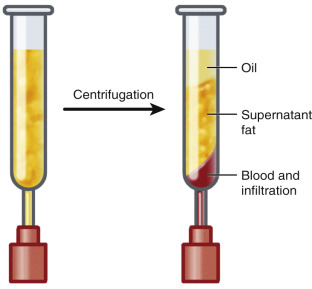
In centrifugation, the lipoaspirate is loaded into 10-mL syringes and centrifuged at ~3000 rpm for approximately 3 minutes. After centrifugation, three layers demarcate: the most inferior portion contains blood, plasma, and local anesthesia, which are drained from the base of the syringe. The middle layer is comprised of adipocytes, which are ultimately grafted. The top layer is a lipid-rich layer that can be poured off and is then wicked with cotton gauze for further removal of oil ( Fig. 20.2 ).
Related posts:
 Immediate Implant Breast Reconstruction With Total Muscle Coverage – Two-Stage
Immediate Implant Breast Reconstruction With Total Muscle Coverage – Two-Stage
 Free Transverse Upper Gracilis Flap Breast Reconstruction
Free Transverse Upper Gracilis Flap Breast Reconstruction
 Partial Breast Reconstruction With Local Tissue Rearrangements
Partial Breast Reconstruction With Local Tissue Rearrangements
 Immediate Prepectoral Implant Breast Reconstruction
Immediate Prepectoral Implant Breast Reconstruction
 Fat Grafting for Total Breast Reconstruction
Fat Grafting for Total Breast Reconstruction
 Partial Breast Reconstruction With Flaps
Partial Breast Reconstruction With Flaps
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


