Fasciotomy of the Thigh, Lower Leg, and Foot
Graeme E. McFarland
Jason T. Lee
DEFINITION
Fasciotomy is indicated to treat compartment syndrome and prevent nerve injury and myonecrosis.
Compartment syndrome most often occurs in the setting of reperfusion of an acutely ischemic limb or in severe limb trauma.
Compartment syndrome can also occur in the setting of occlusive deep vein thrombosis (DVT) of the iliofemoral veins resulting in phlegmasia.
Fasciotomy is indicated for treatment of active compartment syndrome, prophylactically for patients at high risk for compartment syndrome, or for those in which a reliable exam is difficult to obtain (ie, head trauma) and heightened concern for compartment syndrome.
Isolated compartment syndrome of the thigh is rare and often due to femur fracture. The anterior compartment of the thigh is most commonly involved.1
ANATOMY
There are three fascial compartments of the thigh all surrounded by the strong fascia lata.
Anterior:
Muscles: Sartorius, articularis genus, rectus femoris, vastus lateralis, vastus intermedius, and the vastus medialis
Neurovascular: Femoral nerve
Medial (adductor):
Muscles: Adductor longus/brevis/minimus, gracilis, pectineus, and external obturator
Neurovascular: Obturator nerve
Posterior:
Muscles: Adductor magnus, biceps femoris, semitendinosus, and semimembranosus
Neurovascular: Sciatic nerve
There are four fascial compartments of the lower leg.
Anterior:
Muscles: Tibialis anterior, extensor hallucis longus, extensor digitorum longus, and the peroneus tertius
Neurovascular: Anterior tibial artery and vein and the deep peroneal nerve
Lateral:
Muscles: Fibularis longus/brevis
Neurovascular: Superficial peroneal nerve
Superficial posterior:
Muscles: Gastrocnemius, soleus, plantaris
Neurovascular: Tibial nerve
Deep posterior compartment:
Muscles: Tibialis posterior, flexor hallucis longus, flexor digitorum longus, and popliteus
Neurovascular: Tibial nerve, posterior tibial artery and veins, and the peroneal artery and veins
There are technically nine compartments of the foot.
Medial compartment:
Muscles: Abductor hallucis and flexor hallucis brevis
Lateral compartment:
Muscles: Flexor digiti minimi brevis and abductor digiti minimi
Superficial central compartment:
Muscles: Flexor digitorum brevis
Central central compartment
Muscles: Quadratus plantae
Deep central compartment
Muscles: Adductor hallucis compartment
Intrinsic compartment:
Muscles: Four intrinsic muscles (compartments) between the 1st and 5th metatarsals
DIAGNOSIS
Compartment syndrome can be diagnosed by directly measuring the compartment pressures with a Stryker monitor set or with an arterial line transducer system.
Compartment pressures greater than 30 mm Hg are indicative of compartment syndrome.
The “6 P’s” of the compartment syndrome exam are pain, paresthesia, paresis, pallor, pulselessness, and poikilothermia.
“Pain out of proportion to examination” and pain with passive flexion are the most consistent signs of compartment syndrome.
A clinical suspicion for compartment syndrome warrants surgical intervention regardless of compartment pressure measurement.
Paresthesias and paresis are late signs of compartment syndrome and are indicative of poor functional outcomes.
Severe pain of the foot along with dorsal swelling can indicate compartment syndrome of the foot.2
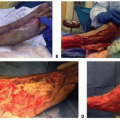
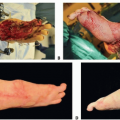
TECHNIQUES
▪ Thigh Fasciotomy (TECH FIG 1)
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


