5 Eyes
Summary
This chapter focuses on the principles and surgical techniques associated with reconstruction of defects involving the eye. Eyelid reconstruction seeks to provide adequate eyelid function and globe protection while maintaining acceptable cosmetic result. Eye reconstruction is broken up into subunits, with different treatment algorithms for upper compared to lower eyelid defects that are normally based on defect size. Of further importance, we discuss the evaluation of canthal tendon integrity and reconstruction with respect to lateral and medial canthal injuries.
Keywords: tarsus, canthal tendon, anterior lamella, posterior lamella, skin graft, cutler-beard flap, tarsal conjunctival flap, gray line, canthoplasty
 Introduction
Introduction
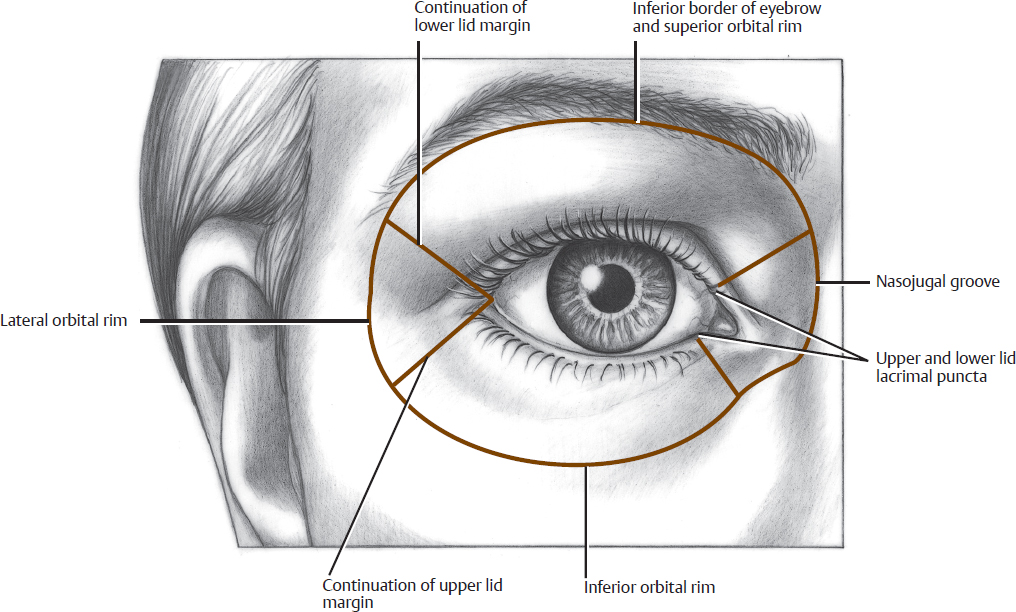
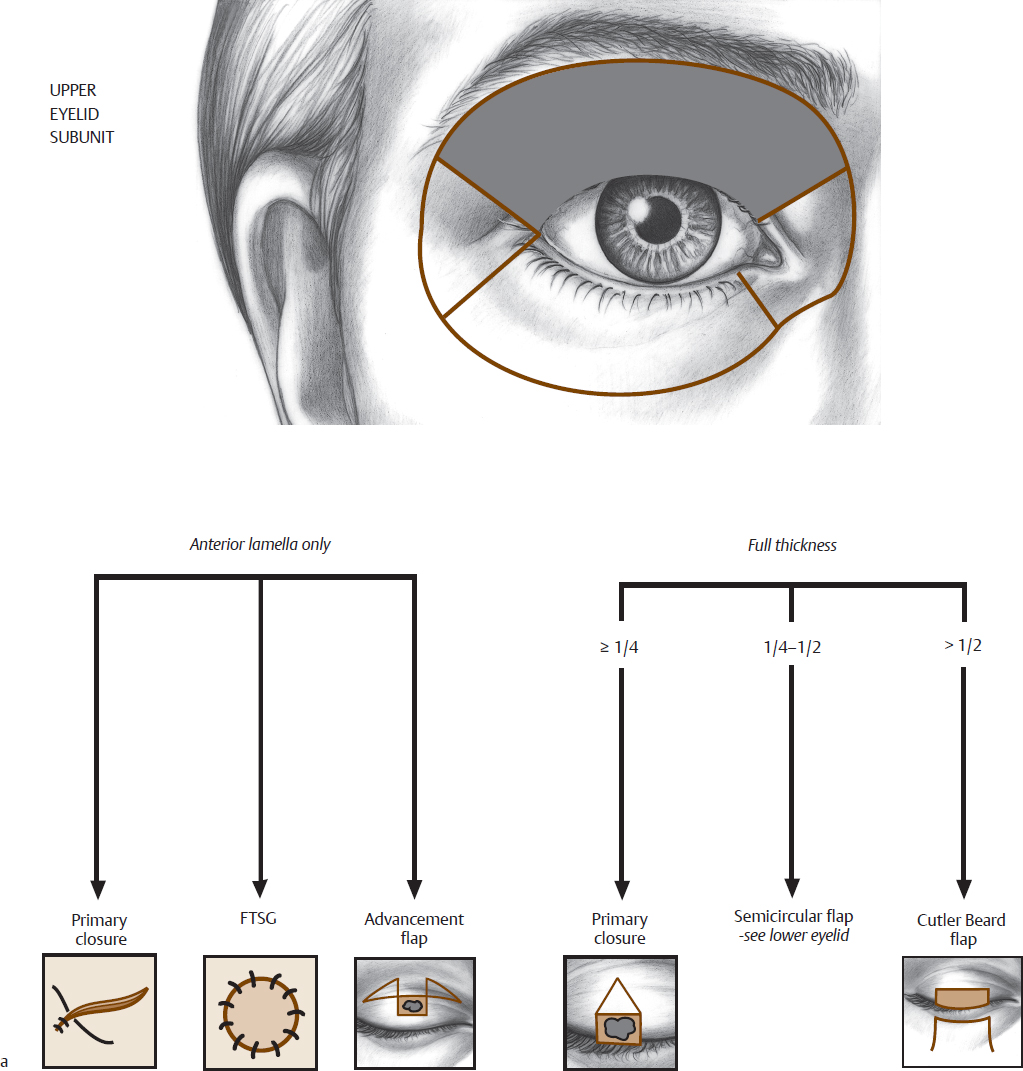
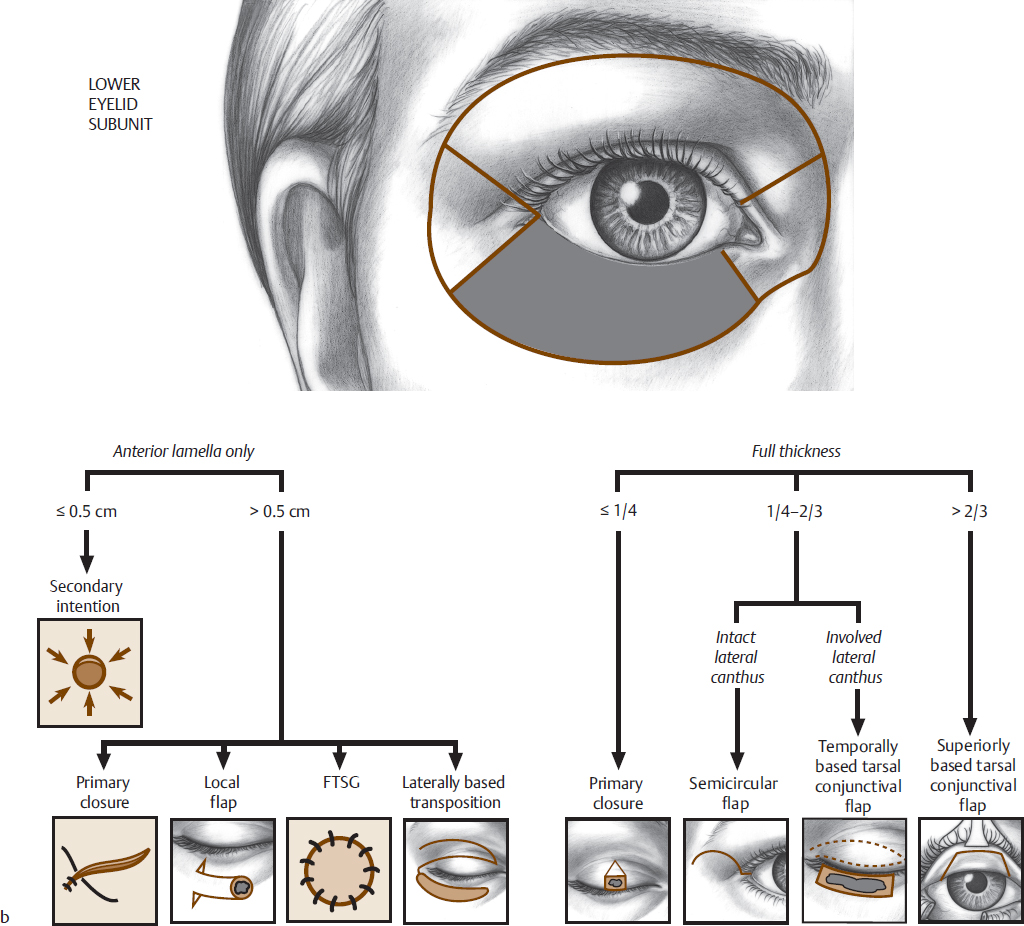
In periocular reconstruction, the surgeon must provide adequate eyelid function, globe protection, and aesthetically acceptable results. The anatomical boundaries of the periocular aesthetic unit are the inferior border of the eyebrow, the lateral and inferior orbital rim, and the nasojugal groove (Fig. 5.1). The periocular region can be divided into four subunits: the lower eyelid, the upper eyelid, the medial canthal region, and the lateral canthal region. The upper and lower eyelids are divided superficially deep into the anterior lamella, containing skin and the orbicularis oculi muscle, as well as the posterior lamella of the conjunctiva, tarsi, and lid retractors. The medial canthal subunit is concave and contains the lacrimal drainage system and the medial canthal tendon. The lateral canthal subunit is slightly concave and contains the lateral canthal tendon. The eyebrow is treated as a subunit of the forehead, as its skin thickness, elasticity, and contour better match this region.
 Upper and Lower Eyelids
Upper and Lower Eyelids
The upper and lower eyelids are separated into four categories for repair: anterior lamellar defects, and full-thickness defects involving <25% of the lid, 25–50% of the lid, and >50% of the lid. Full-thickness defects of the upper and lower eyelids must be reconstructed in multiple layers for optimal function and appearance. Each category will be discussed in detail for the upper and lower lids, along with the medial and lateral canthus.
 Upper Eyelid
Upper Eyelid
Anterior Lamellar Defects
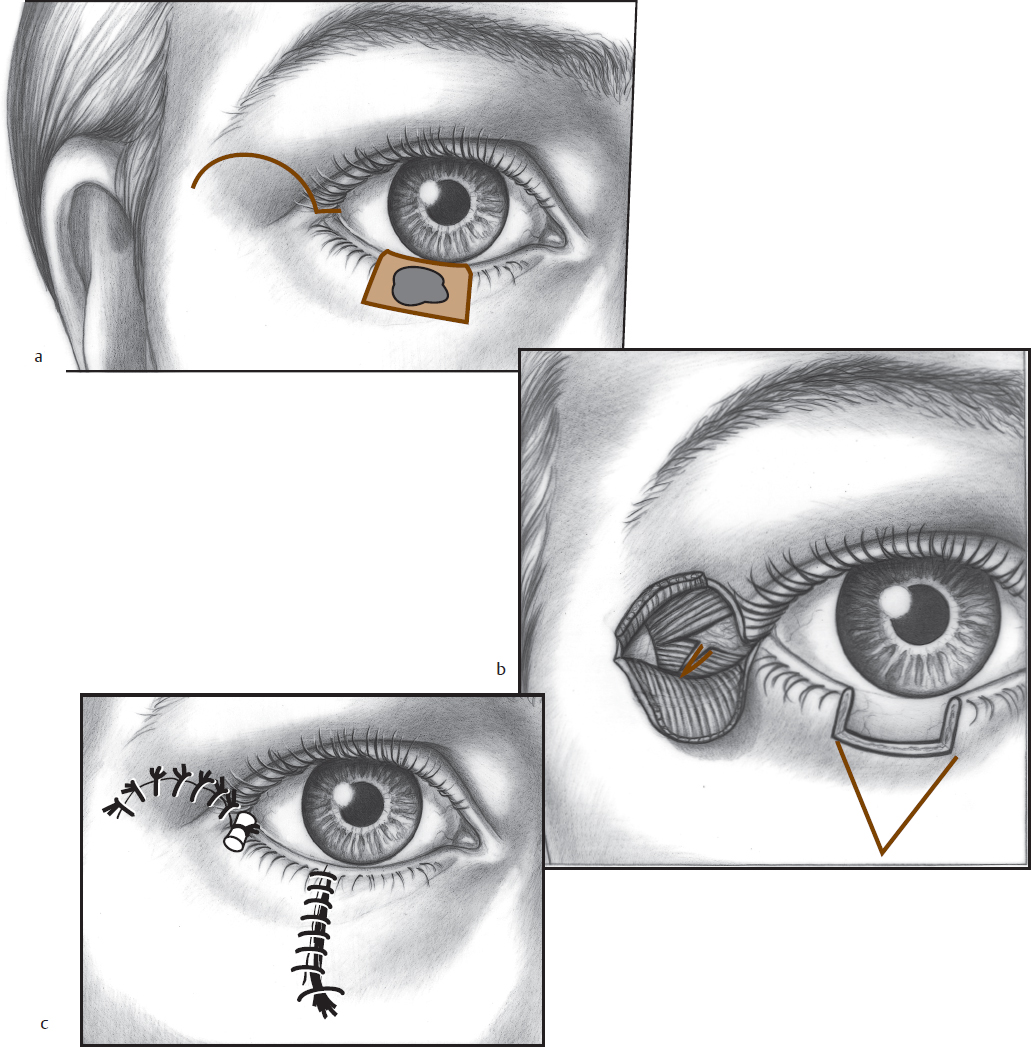
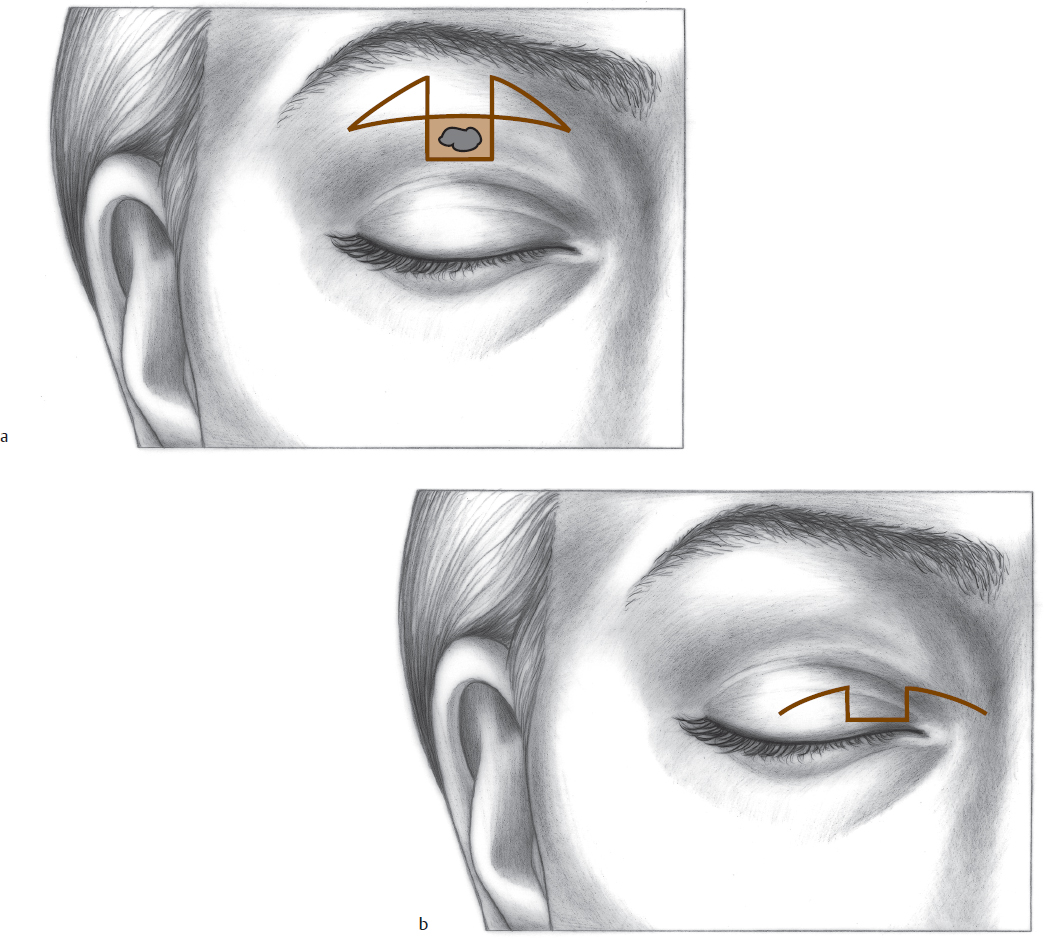
A partial-thickness defect of the upper or lower eyelid <0.5 cm in diameter heals well by secondary intention (Fig. 5.2). A defect <50% of the anterior lamella of the upper eyelid can be closed with a variety of local flaps. Upper eyelid defects are best closed with flaps incised parallel to the natural creases of the eyelid (Fig. 5.3). The orbicularis muscle is removed from the deep surface of the defect. The flaps are harvested as skin–muscle flaps. Care must be taken to avoid excessive tension on the closure. The muscle is closed with 6–0 or 7–0 buried absorbable sutures, and the skin is closed with a 6–0 or 7–0 monofilament suture. If excess tension causes lagophthalmos or ectropion, other tissues must be brought into the area for proper reconstruction.
Full Thickness < 25%
Defects up to 25% of the upper or lower eyelid can be closed primarily (Fig. 5.4, Fig. 5.5, and Fig. 5.6). The incision through the tarsal plate is perpendicular to the lid margin. A full-thickness Burow triangle is incised away from the edge of the tarsal plate, farthest from the lid margin. The first suture of 6–0 silk is placed precisely at the lid margin (“gray line”), entering the skin 3 mm from the cut edge, to a depth of 3 mm, and exiting 3 mm from the opposite cut skin edge. Two or three 6–0 absorbable sutures with the knots superficial are then used to approximate the tarsus. The anterior lid margin is closed with 6–0 silk sutures left long, so they can be tied away from the lid margin under the most distal suture. An alternative is to use a buried mattress absorbable suture at the margin. The skin sutures are removed in 4 or 5 days and the lid margin sutures in 7 to 10 days.
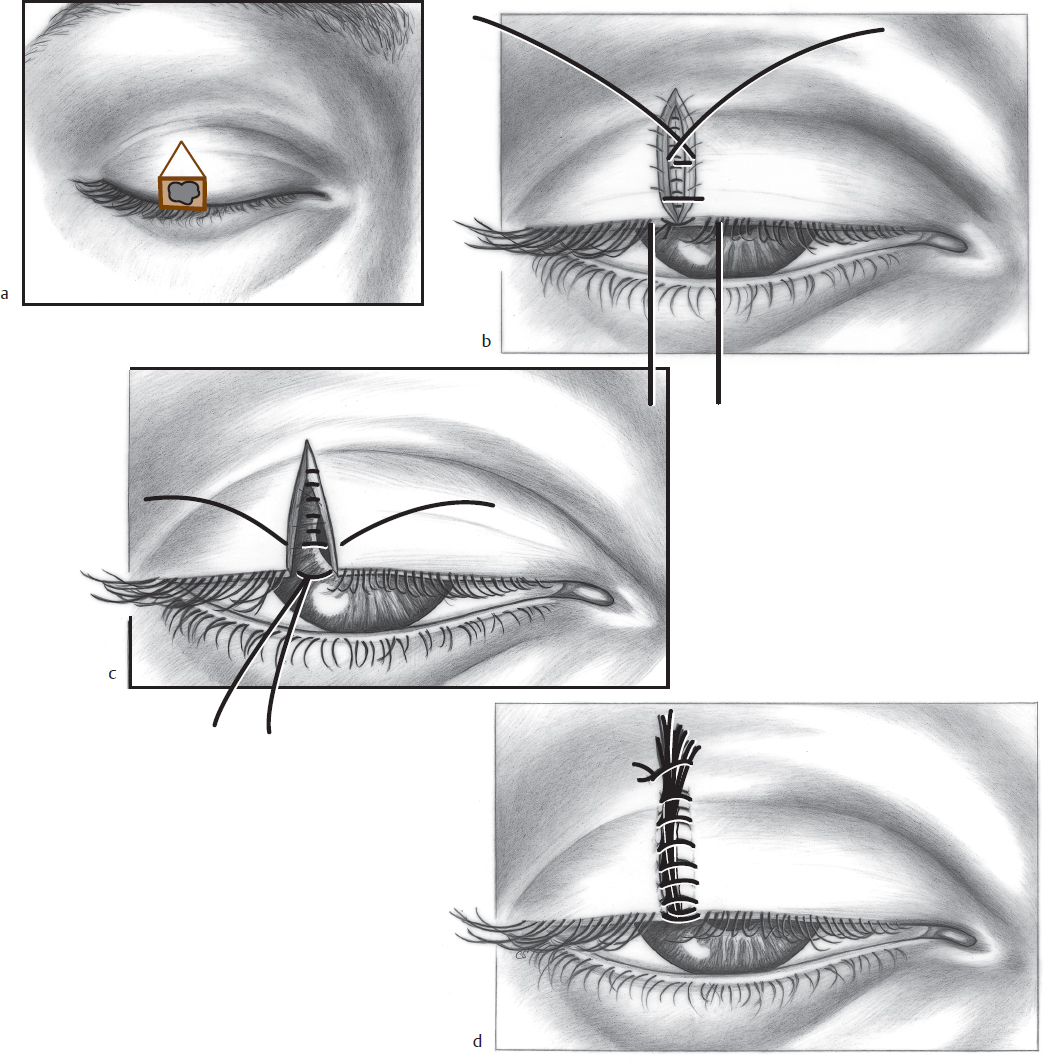
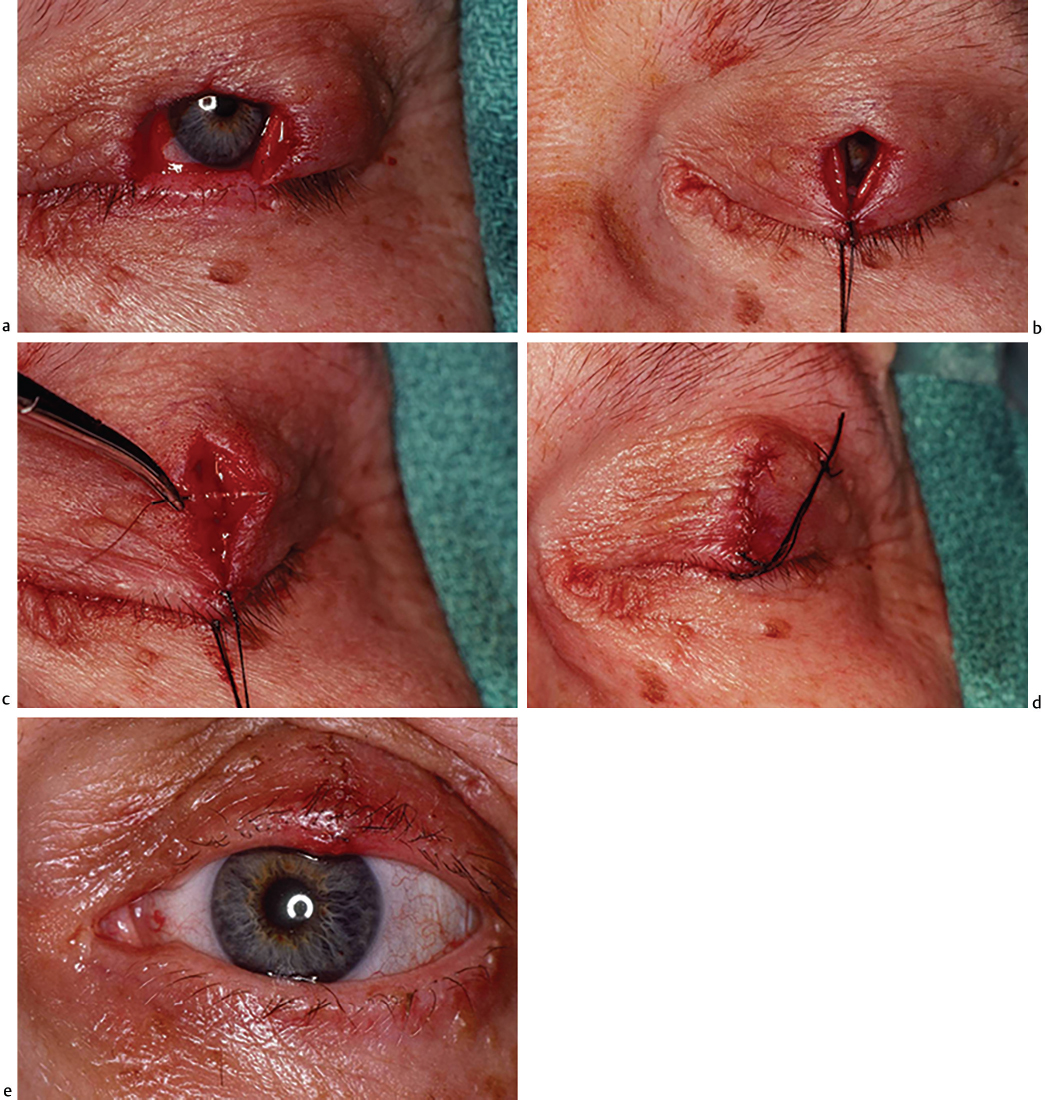
Fig. 5.5 (a) Full-thickness upper eyelid defect (<25%). (b) Primary closure of the eyelid with the first suture placed at the lid margin. (c) Approximation of the tarsus. (d) Closure of the anterior lid margin. (e) Early postoperative appearance.
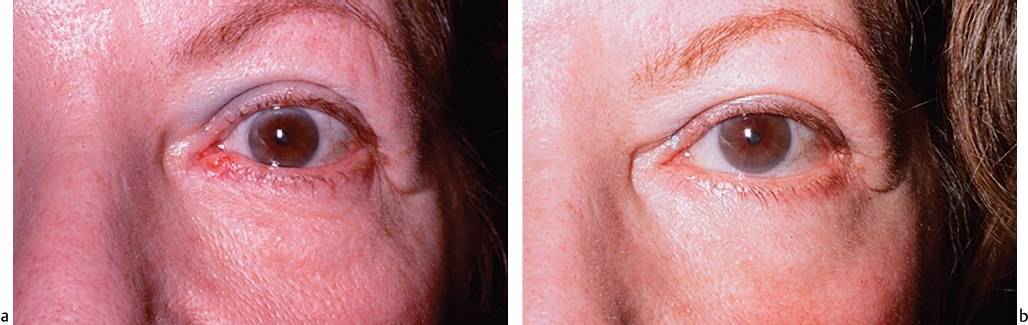
Fig. 5.6 (a) Basal cell carcinoma of the left medial lower eyelid. (b) One year after full-thickness primary lower lid closure.
Full Thickness 25–50%
Up to one-half of the upper lid can be closed with the semicircular flap (Fig. 5.7 and Fig. 5.8). The lateral canthus must be intact for utilization of this flap. The defect site is prepared, as in the primary closure case, with a Burow triangle excision at the base of the defect (“inverted house”), away from the tarsus. A semicircle, starting at the lateral canthus, and in the opposite direction from the lid involved, is drawn. For the lower lid, the semicircle is kept within the outlines of a line that would be an inferior continuation of the eyebrow. A skin flap is incised to the depth of the lateral orbital rim periosteum. The lateral canthal tendon is identified, and the limb to the involved eyelid is cut at the orbital rim. The defect edges are then approximated by pulling on the cut edges with skin hooks. Upper eyelid defects should be repaired with less tension, or ptosis will result.
If there is excessive tension at the first approximation of wound edges, then the orbital septum, lid retractors, and conjunctiva can be sequentially cut to relieve tension. Once appropriate tension is obtained, the primary defect site is closed, as previously described, for primary closure of full-thickness defects. The lateral canthus is reformed with a vertical mattress 5–0 or 6–0 monofilament suture tied over a bolster. This suture is placed beginning at the skin surface of the normal lid and passing full thickness through first the normal and then the involved lid. The short limb of the vertical mattress suture is passed from the involved lid to the normal lid and includes the intact limb of the lateral canthal tendon. This suture is left in place 7 to 10 days. The rest of the semicircular flap is closed, using the principle of halving, with vertical mattress sutures.