8 Ears
Summary
This chapter focuses on the specific considerations with respect to ear reconstruction. Ear reconstruction is classically complex, given the cartilage framework and intimate relationship of the skin with the perichondrium. This chapter provides a reconstruction algorithm based on the defect location from more basic primary closure of earlobe defects, to complete reconstruction using cartilage grafting and staged flaps. Specific attention is also provided with respect to the intimate relationship of perichondrium and reconstruction choice.
Keywords: helical advancement, tubed pedicle flap, helical rim, concha, bolster, star wedge excision, postauricular flap, cartilage harvest
The ear is composed of a framework of unique elastic cartilage that is extremely flexible. Laterally, this framework is covered by an inelastic, thin skin with scant, underlying subcutaneous tissue. The skin on the lateral ear is adherent to the perichondrium and thus reveals the contours of the underlying ear cartilage in great detail. On the medial surface, the skin has a greater amount of subcutaneous tissue and is much less adherent to the underlying perichondrium. Because of the extremely complex contour of the auricle, subunit division and reconstruction are not practical. Rather, the ear is more effectively divided by areas of concavity or convexity in considering reconstruction (Fig. 8.1).
Cartilage present in the concavities of the ear is less critical to the appearance of the ear and can be used as grafting material for other areas of the face. Cartilage grafts from the conchal bowl can be used for nose and eyelid reconstruction. Composite grafts from the superior helix are of value for nasal reconstruction. Cutaneous-perichondrial grafts from the conchal bowl are useful for nasal reconstruction; these grafts of skin and perichondrium can be used to repair partial-thickness defects of the ala and will contract minimally.
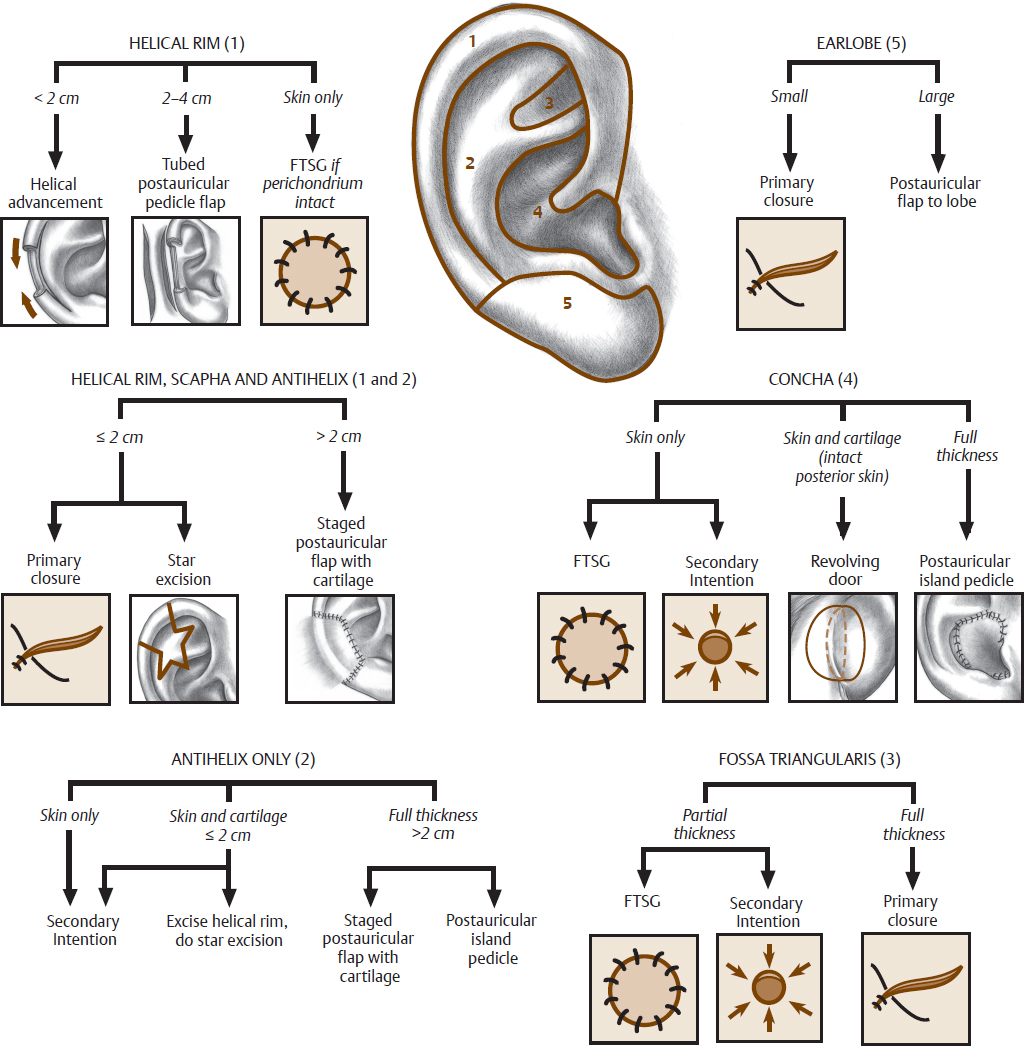
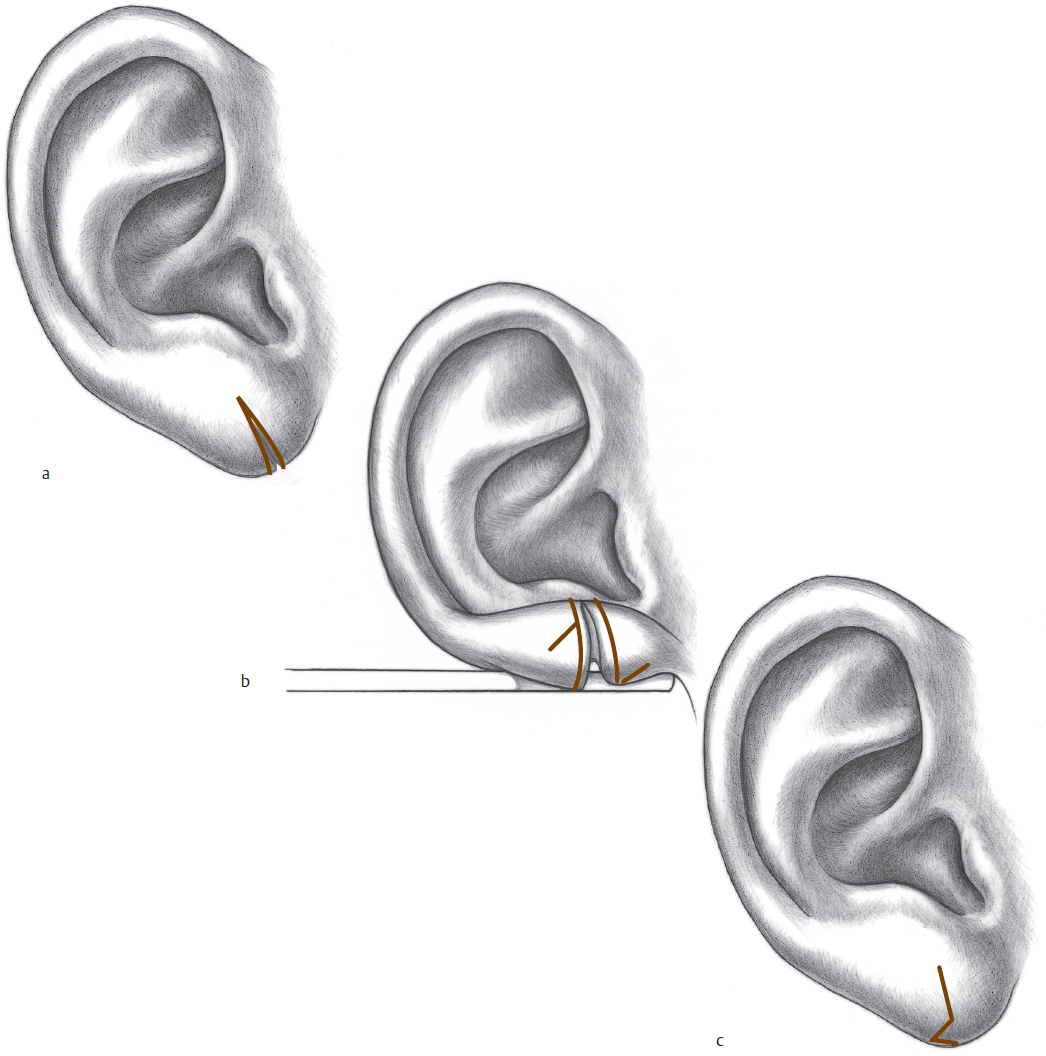
The location, depth, and size of the ear defect are all factors that must be considered in choosing appropriate reconstructive options. Defects that involve skin only and are located in a concave region of the ear can often be allowed to heal by secondary intention with acceptable cosmetic results. Skin defects overlying convexities tend to heal less well by secondary intention, though some patients will accept the results to avoid surgery. Small defects over a convexity of the ear can be repaired with a full-thickness skin graft (FTSG) or by mobilization of adjacent skin from a concave region, which can, in turn, be allowed to heal by secondary intention (Fig. 8.2).
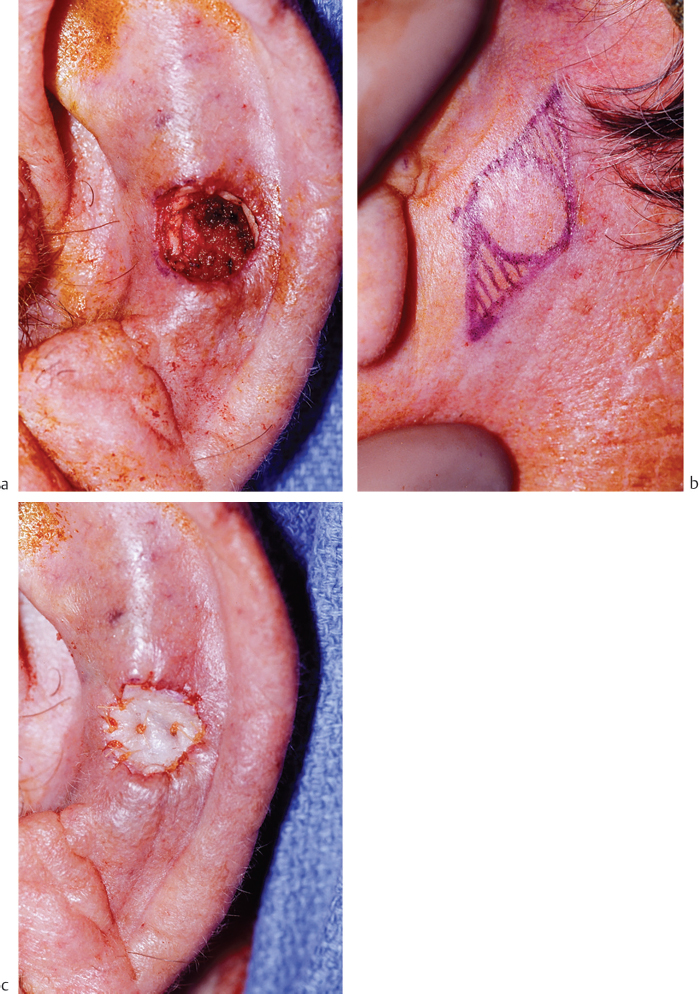
Fig. 8.2 (a) Defect of a convex portion of the ear. (b) Postauricular skin is a good donor site for full-thickness skin grafts (FTSGs). (c) FTSG sewn into place.
Defects of the concha that include loss of anterior skin and cartilage can be treated with either an FTSG or a “revolving door” postauricular flap (Fig. 8.3 and Fig. 8.4). The “revolving door” flap recruits the postauricular skin as an island pedicle flap to reconstruct the anterior concha. Approximately one-third of the skin is taken from the back of the auricle and two-thirds from the skin posterior to the sulcus. The donor site is closed primarily.
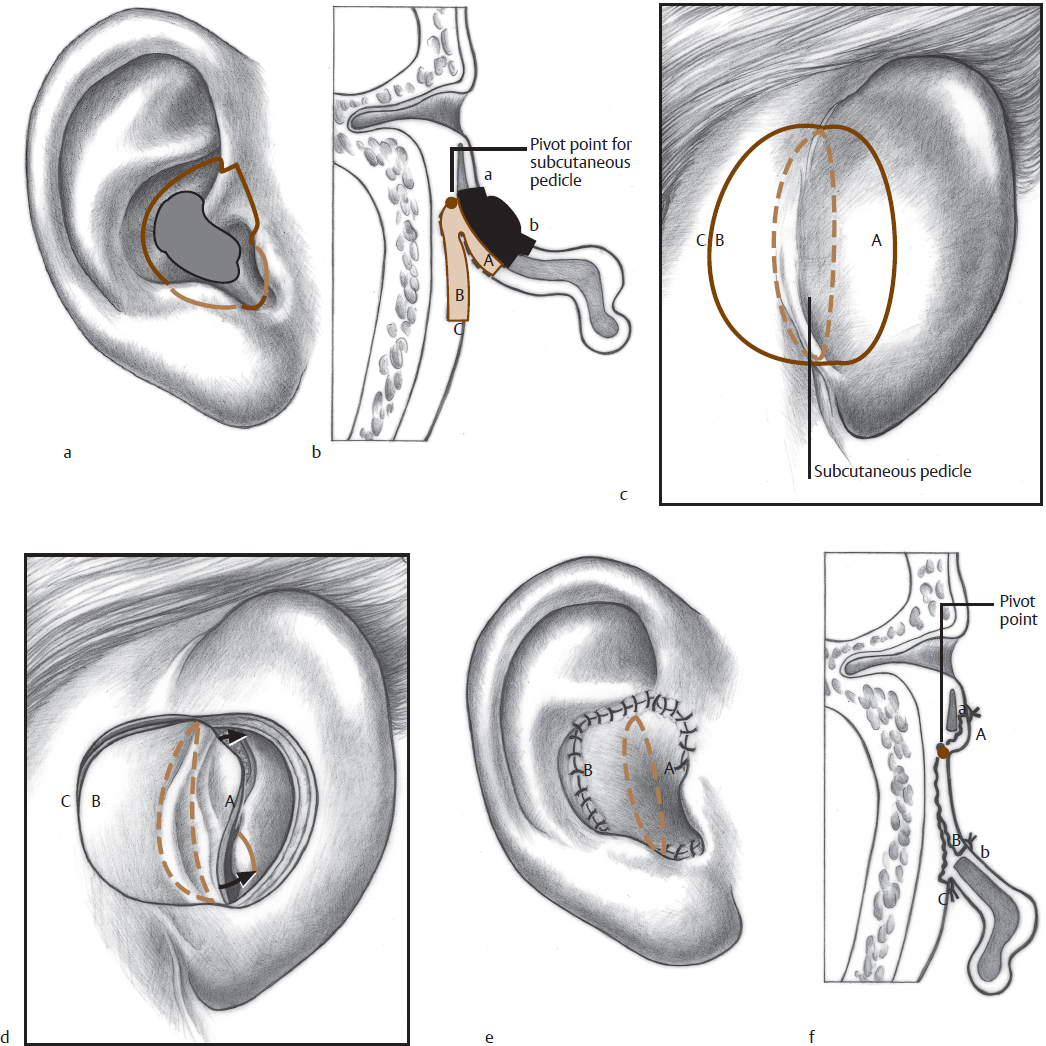
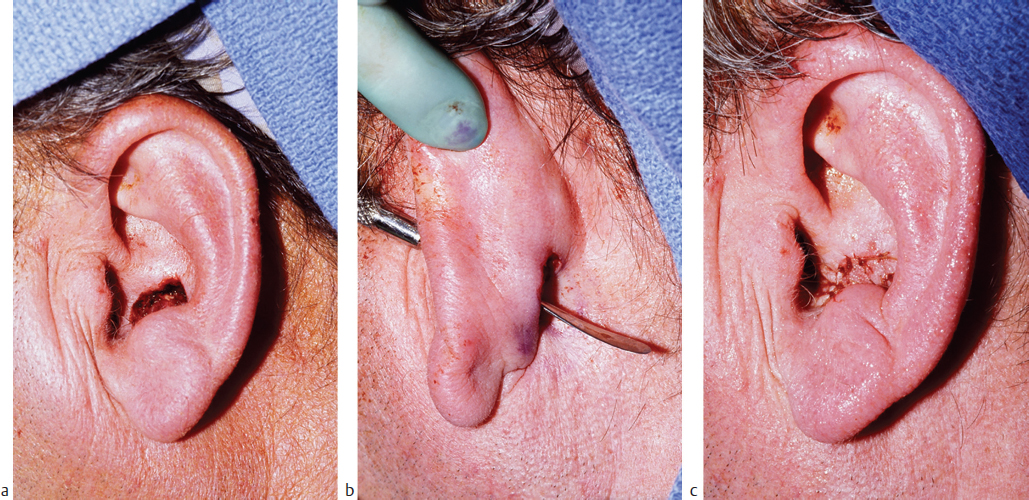
Fig. 8.4 (a) Conchal bowl defect involving anterior skin and cartilage. (b) A through-and-through defect is produced after an incision is made in the postauricular skin, and the flap is pulled forward into the defect. (c) The flap is sewn in place, and the postauricular skin is closed onto itself.
Skin-only defects involving the helix or ear margin may be repaired with local skin flaps from the adjacent postauricular surface. Such defects of the lobule or anterior helix can be repaired with a one-stage flap, whereas defects on the midportion may require a staged procedure, with severance of the flap base at 3 weeks.
A tear of the earlobe is common and is usually secondary to an earring pulled through the base of a pierced ear. A simple closure may result in notching at the earlobe margin; therefore, a small Z-plasty is incorporated in the repair (Fig. 8.5). Each limb of the Z-plasty only needs to be the width of a no. 15 blade. The patient should not pierce the ear for 3 to 6 months postoperatively, or the defect may recur. Clip-on earrings can be worn in the interim.