23. Lateral Canthal Complications in Aesthetic Eyelid Surgery: Prevention and Reconstruction
23.1 Introduction
The lateral canthus is an important aesthetic facial landmark. It is formed by fusion of the upper and lower tarsal plates and is supported by muscular and fibrous lateral orbital attachments (Fig. 23.1). The posterior limb of the canthal tendon (lateral palpebral ligament) anchors the tarsi to the internal zygoma at the lateral orbital tubercle (Whitnall’s tubercle) (Fig. 23.2). The comparatively diminutive anterior limb interdigitates with the orbicularis oculi muscle. In addition to supporting the lower eyelid, it limits medial displacement of the tarsi during blinking.


Age-related attenuation of the canthal constituents, particularly the tarsoligamentous, imparts laxity to the lower eyelid. Unrecognized or untreated lower lid laxity may contribute to well-recognized deformities after aesthetic eyelid surgery, such as the round-eye syndrome, canthal malposition, and scleral show. Functional consequences may also result if eyelid blink and tear drainage are compromised. An extensive literature describes these multifaceted problems and viewpoints regarding their diagnosis and treatment. 1 , 2 , 3 , 4 , 5 , 6 , 7 , 8 This chapter describes the prevention or reconstruction of these complications.
23.2 Lateral Canthal Morphology
The lateral canthus is typically higher than the medial; thus, the lid ascends over its course from the medial to lateral osseous attachment. Exceptions occur, however, and comparison of photographs from a younger age with preoperative pictures is valuable in assessing age-related or postoperative position changes.
23.3 Lid Laxity: Evaluation
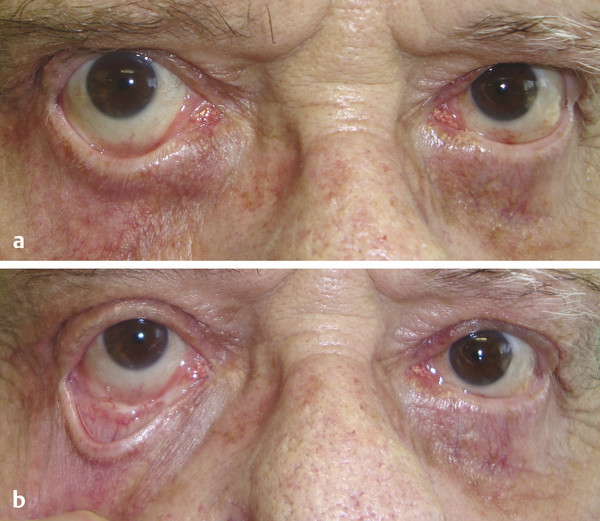
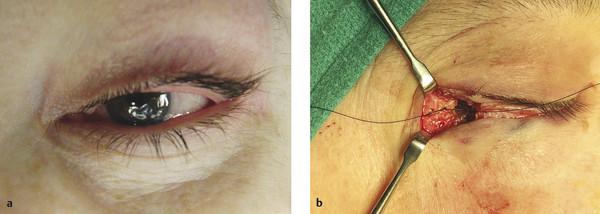
Lower eyelid shape and appearance at the canthal angle are important indicators of orbicularis oculi muscle tone and tarsotendinous status. A crescent-shaped lower lid contour or lower lid descent at the lateral limbic line implies anterior lamella laxity, possible orbicularis atrophy, and tendon dehiscence (Fig. 23.3). Frank ectropion (Fig. 23.4 a) or failure of the lid to return to the globe after downward displacement (without blinking) establishes advanced laxity of both muscular and eyelid ligamentous elements (Fig. 23.4 b). Horizontal fissure effacement (i.e., phimosis) and widening of the lateral canthal angle indicate tarsotendinous separation at the lateral orbital rim.

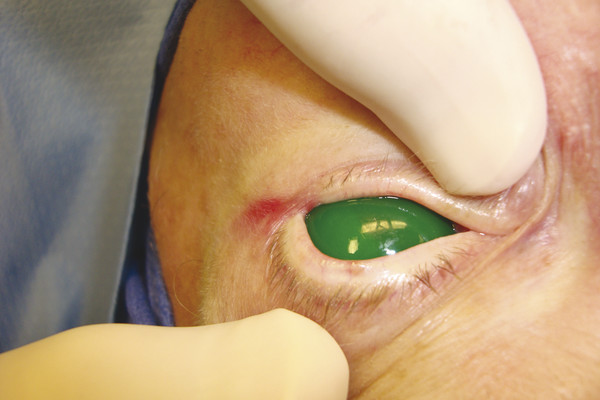
The foregoing changes in lid and canthal morphology alert the surgeon to eyelid laxity during preoperative examination. Intraoperative evaluation definitively refines its cause and degree. Thinning of the lower lid margin at the raphe indicates tarsal distraction from the tendon (Fig. 23.5). If the lateral eyelid can be displaced no farther than the plane of the medial aspect of the lateral rim, tarsal laxity is mild. Eyelid translation beyond this plane indicates moderate to severe loss of tension and mandates tarsotendinous reconstruction and orbicularis tightening, as discussed in the following section (Fig. 23.6).

23.4 Lid Laxity: Treatment
Numerous techniques restore tarsotendinous tension. Bick’s tarsal resection improves eyelid tension and does not disrupt the canthus. 8 , 9 Shortening of horizontal fissure length and increased tension on tendon attachment to the tarsus, with the attendant risk of recurrent laxity, are disadvantages.
The tarsal strip technique re-creates a neocanthal tendon from the terminal lower tarsus. 10 It is effective and avoids Bick’s disadvantages but may misalign the upper and lower eyelids. Alternatively, direct reapproximation of both the terminal upper and lower tarsi to the periosteum at Whitnall’s tubercle restores tension while preserving the eyelid’s lateral anatomical relationships (see later). It also permits vertical modification of canthal position relative to the medial canthus.
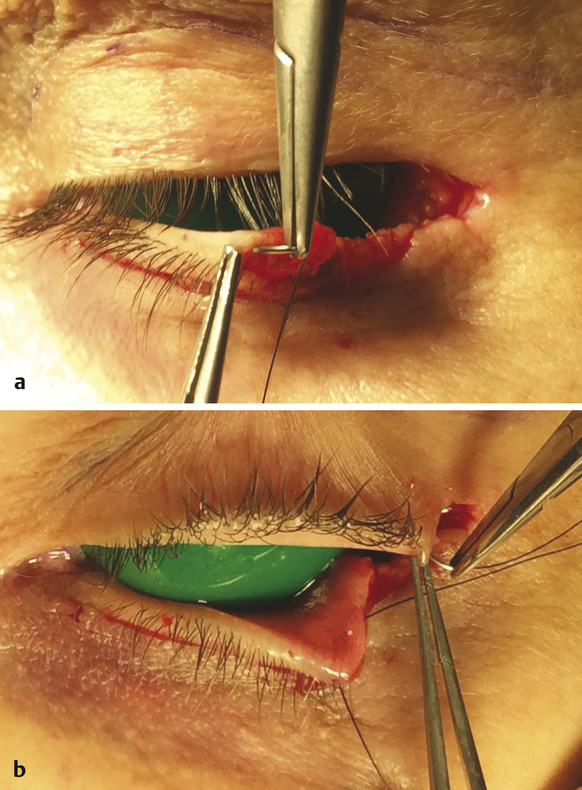
Mild laxity requires only suture fixation of the tarsi to the periosteum at Whitnall’s tubercle, as discussed later herein. Moderate to severe laxity is treated by tarsal resection. The amount of tarsal resection required is assessed by the lateral translation maneuver: the osseous attachments of lower tarsus (posterior canthal tendon, capsulopalpebral fascia, orbital septum) are first released from the canthal tendon, and the tarsus is drawn laterally with moderate tension. Tarsus extending beyond the plane of the medial aspect of the lateral orbital wall is resected (Fig. 23.7).

To re-create the tarsoperiosteal attachment, a double-armed 5–0 nylon (Ethicon S-22) (preferred) or 4–0 Polydek (Deknatel ME-2) enters the terminal tarsus of the lower eyelid and then the upper eyelid (Fig. 23.8). The needles consecutively purchase the soft tissue overlying the lateral tubercle on the correct vertical plane (typically slightly higher than the medial canthal tendon) (Fig. 23.9). From this coordinate, they scythe anteriorly along the orbital wall periosteum, exiting the soft tissue at the orbital margin (Fig. 23.10 a).
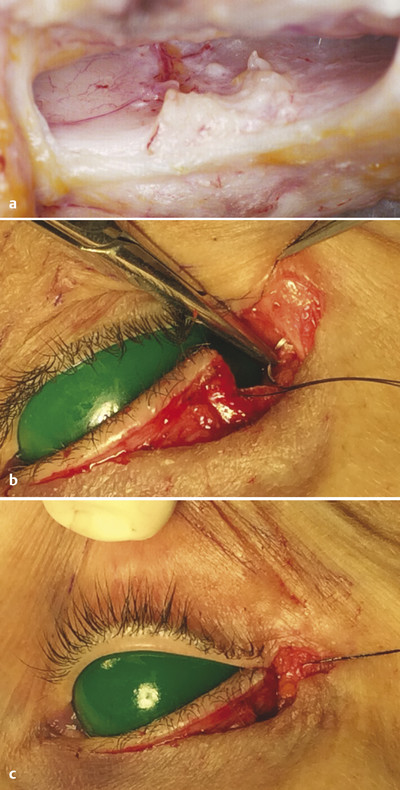
Positioning the fixation suture at the lateral orbital tubercle ensures correct eyelid contact with the globe. Although tissue is usually adequate for suture fixation at this point, periosteal degloving or atrophy may prevent secure fixation. In this case, the tarsi are anchored by drilling two holes in the lateral orbital wall that converge to Whitnall’s tubercle. The tarsal sutures are retrieved with a 3–0 wire snare and tied at the lateral rim ( Fig. 23.10 b).
Related posts:
 6. Facial Sculpting and Facial Slimming with Neurotoxins
6. Facial Sculpting and Facial Slimming with Neurotoxins
 20. Comparison of Midface Rejuvenation Techniques
20. Comparison of Midface Rejuvenation Techniques
 22. Lower Eyelid Blepharoplasty
22. Lower Eyelid Blepharoplasty
 5. Energy-Based Treatments for Facial Aging
5. Energy-Based Treatments for Facial Aging
 9. Male versus Female Facelift Surgery. Is There a Difference?
9. Male versus Female Facelift Surgery. Is There a Difference?
 12. Primary Superficial Musculoaponeurotic System (SMAS) Facelift and Neck Lift
12. Primary Superficial Musculoaponeurotic System (SMAS) Facelift and Neck Lift
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


