4 Forehead
Summary
This chapter reviews the fundamental techniques and anatomy associated with forehead defects. The forehead is subdivided into several forehead subunits based on locations. We provide a “decision tree” for treatment based on these subunits with specific attention on whether there is involvement of the hairline or eyebrows.
Keywords: temporal forehead, central forehead, A-to-T Flap, rhombic flap, temple, frontalis, primary closure
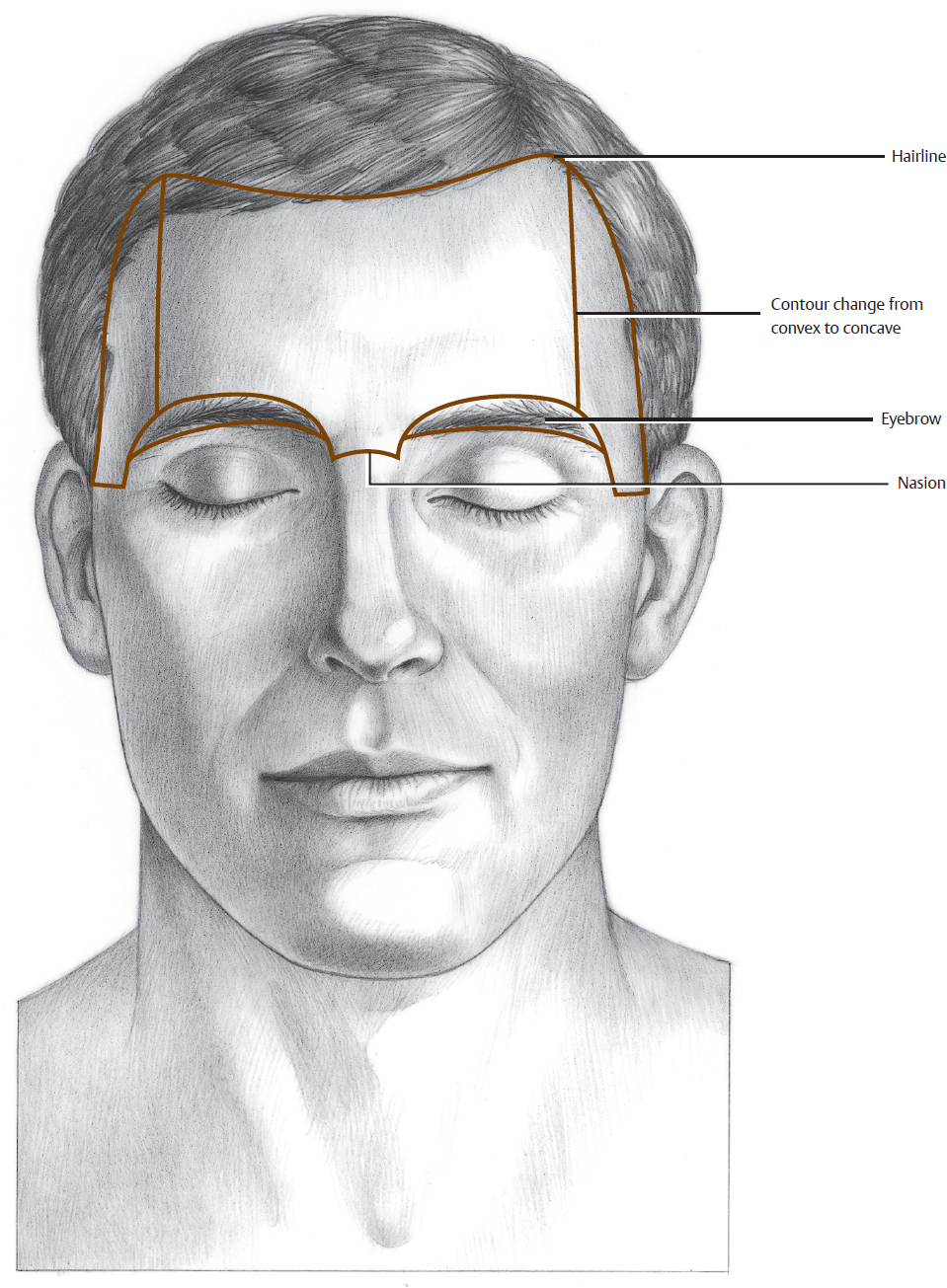
The anatomical boundaries of the forehead unit are the natural hairline (in patients without alopecia), the zygomatic arch, the lower border of the eyebrows, and the nasal root (Fig. 4.1). The upper extent of the forehead unit in patients with alopecia can be identified as the most superior extent of the frontalis muscle. Typically, a distinct superior crease of the forehead marks this spot. The hairline and eyebrows provide camouflaged anatomical boundaries in which to hide incisions. These hair-bearing areas simultaneously limit flap designs to those that do not distort the natural hairline and eyebrow shape.
The forehead unit can be divided into five subunits. Anatomically, the central forehead is an extension of the scalp and retains many similar characteristics. Central forehead skin is thick, rather inelastic, and tightly adherent to the underlying frontalis muscle. On either side of the central forehead is the lateral forehead or temple region, which is more elastic and often acts as a reservoir of tissue for reconstruction. The frontalis muscle is not present in the temple, and the skin is loosely attached to the underlying temporalis fascia. In addition, whereas the central forehead is convex, the temple is somewhat concave. The eyebrows are subunits unto themselves with hair-bearing skin.
The relaxed skin tension lines (RSTLs) run horizontally in the central forehead, as demonstrated by the typical forehead wrinkles. Upon reaching the temporal scalp, they curve in an inferior direction.
Sensory innervation to the central forehead originates from branches of the supraorbital and supratrochlear nerves (Fig. 4.2). Medially, these sensory nerves branch immediately, pierce the overlying muscle fibers, and run superiorly in a superficial subcutaneous plane. More laterally, the nerves run for quite a distance under the frontalis muscle, rather than in the subcutaneous plane. If care is taken when raising flaps, these large sensory branches can be identified and preserved. The origin of the supraorbital nerve can usually be palpated at the foramina in the superior orbital rim border. The supratrochlear neurovascular bundle is usually very close to or within the glabellar creases. This landmark is especially useful when elevating paramedian forehead flaps for nasal reconstruction.
Small defects of the forehead can be closed in a fusiform manner, but a long incision is often required to avoid standing cones at either end; this is preferable to using an M-plasty, which extends outside the RSTLs and is therefore more noticeable. Fusiform repairs should be limited to locations and sizes that do not elevate the eyebrow. Vertical incisions in the central forehead between the medial extent of the brows heal exceptionally well. Midline closures take advantage of the lax tissue in the temple. The M-plasty technique can be used in the inferior extent of a vertical closure, to take advantage of the camouflaging effect of the glabellar wrinkles, and to avoid traversing into the nasal aesthetic subunit.
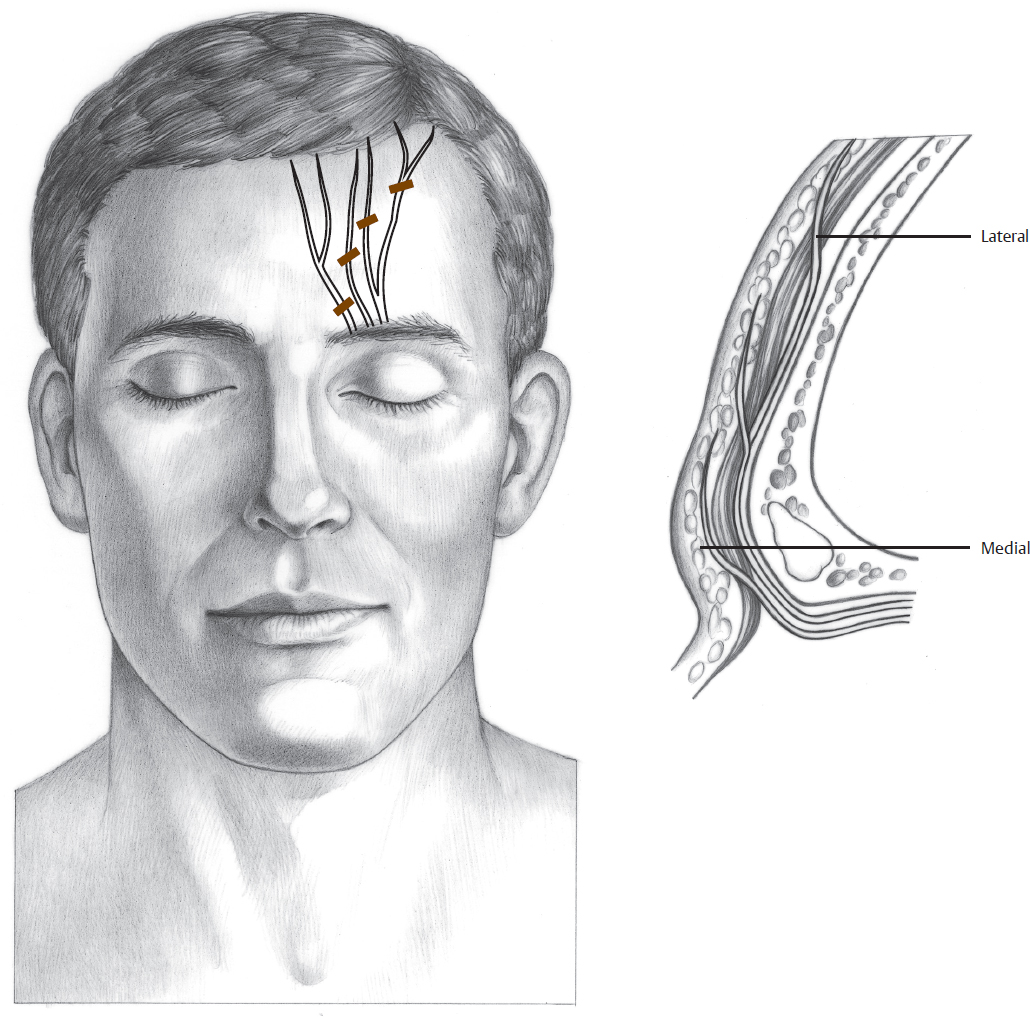
Fig. 4.2 Sensory innervation of the forehead. Adapted with permission from Fatah MF. Innervation and functional reconstruction of the forehead. Br J Plast Surg 1991;44:351–358.
Related posts:
 Liposuction of the abdomen and trunk
Liposuction of the abdomen and trunk
 Physical Medicine and Rehabilitation Management of Children with Congenital Anomalies of the Upper Extremity
Physical Medicine and Rehabilitation Management of Children with Congenital Anomalies of the Upper Extremity
 Patient Selection and Breast Imaging
Patient Selection and Breast Imaging
 Maxillofacial Prosthodontics
Maxillofacial Prosthodontics
 Indications and Techniques for Fat Grafting for Periorbital Rejuvenation
Indications and Techniques for Fat Grafting for Periorbital Rejuvenation
 Nerve Entrapments
Nerve Entrapments
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


