2 Fundamental Techniques
Summary
This chapter reviews such techniques employed in facial reconstruction covering wound closure and care, defect shape, healing by secondary intention, skin and composite grafts, various flaps (advancement, rotation, rhombic, bilobed, and note), Z-plasty, and dermabrasion.
Keywords: skin graft, composite graft, wound closure, secondary intention, advancement flap, rotation flap, rhombic flap, Z-plasty, bilobed flap
 Wound Closure
Wound Closure
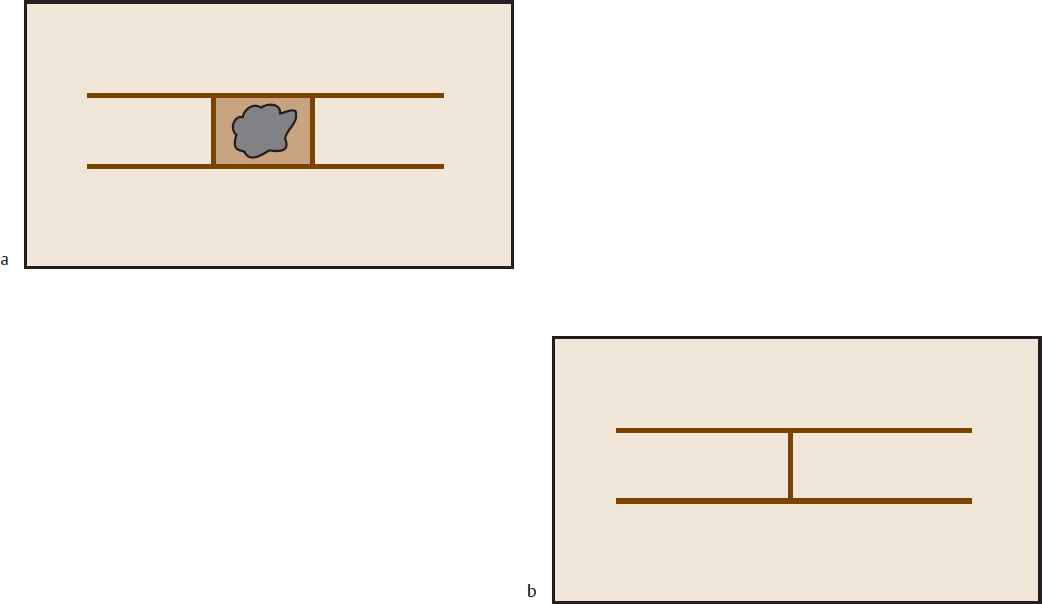
Proper wound closure starts with the initial incision. Incisions should be perpendicular to the skin, except in areas like the scalp, where they are beveled to prevent hair follicle damage (Fig. 2.1). Consult Sherris and Kern’s Essential Surgical Skills (see Suggested Reading) for an in-depth evaluation and hands-on pointers on wound closure techniques. That book especially is useful to the younger student of surgery and will work as an adjunct to the contents of this book. Pearls of wound closure and handling are mentioned in the pages that follow.
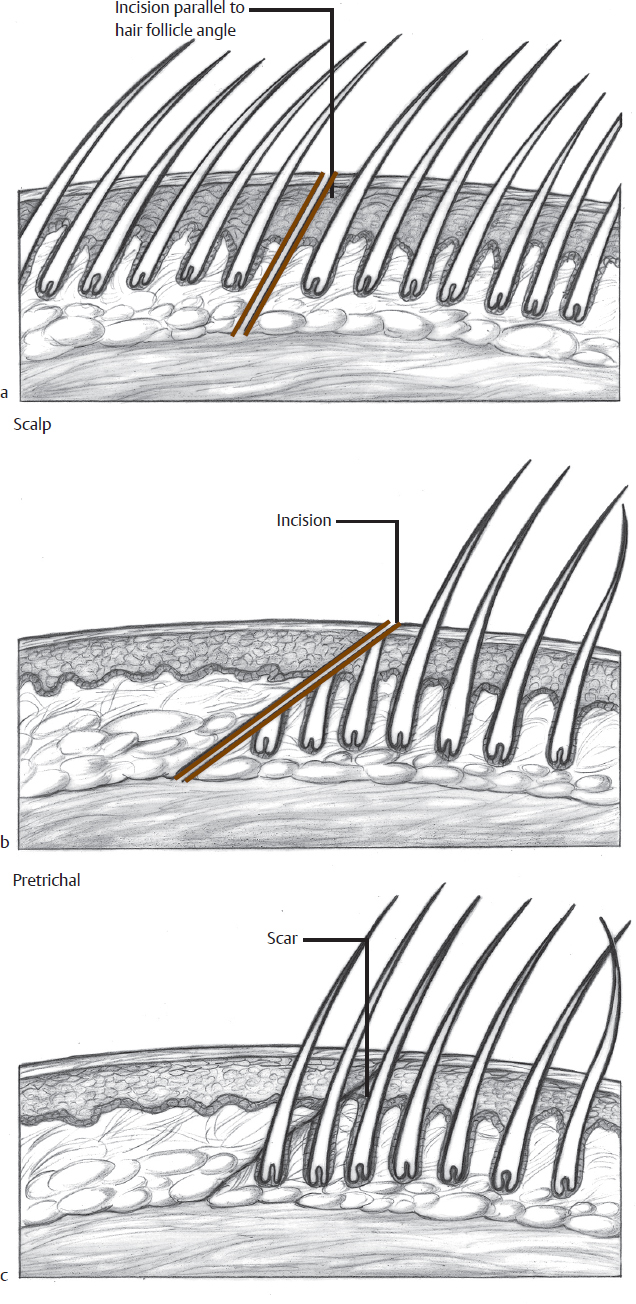
Fig. 2.1 Incisions (a) within the hair and (b) the hairline and (c) growth of hair through the scar.
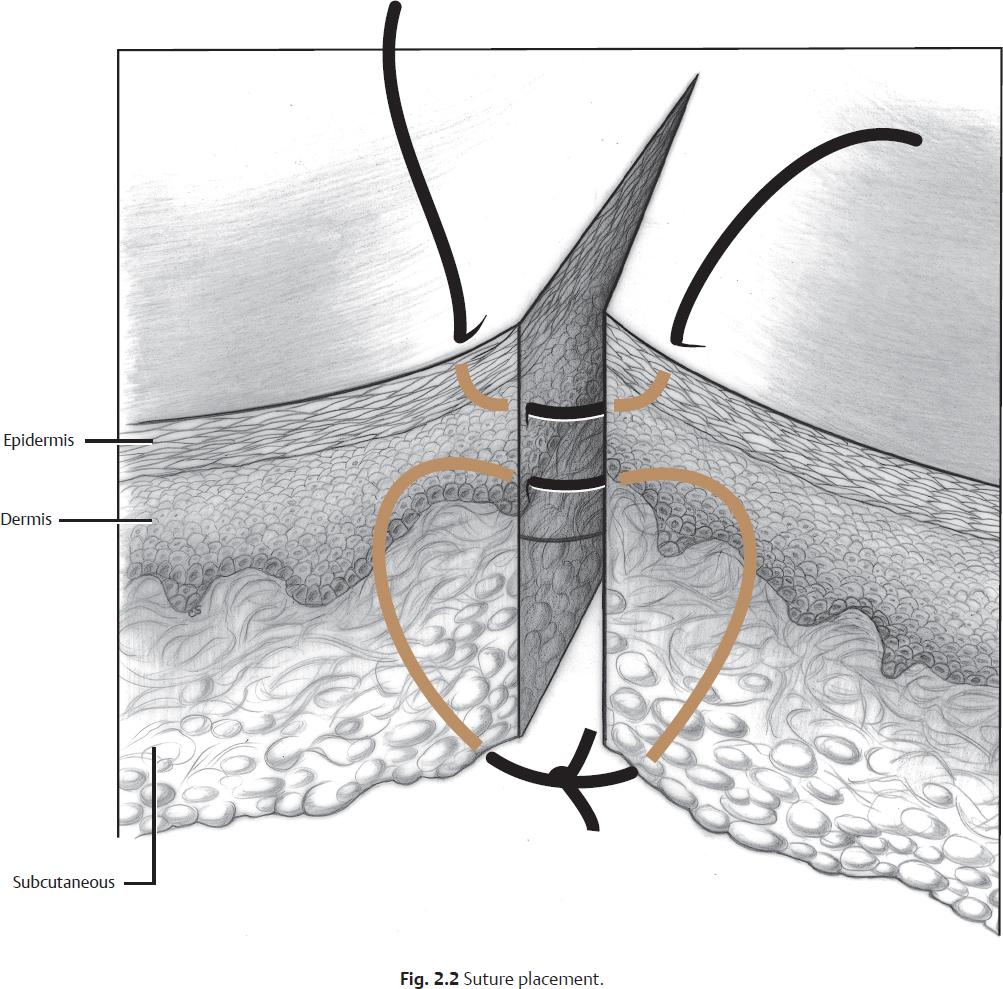
The deep layers of the flap are closed with absorbable suture at the dermal and/or subcutaneous level (Fig. 2.2). The deep closure decreases wound-closing tension, decreases dead space in the wound, and aids in eversion at the skin edge. The skin edge is closed with 5–0 to 7–0 nonabsorbable suture, initiated with the needle perpendicular to the skin. Staples can be used in closure of the hair-bearing scalp after galeal closure.
Standing cone or “dog-ear” deformities commonly occur during flap inset and skin closure (Fig. 2.3). A Burow triangle must be excised to treat these deformities. The simplest method is to hold the cone under slight upward tension and make the first skin cut from the base of the redundant tissue to the apex of the wound, approximately paralleling the relaxed skin tension lines (RSTLs). The excess tissue of the other side is then overlapped and excised.
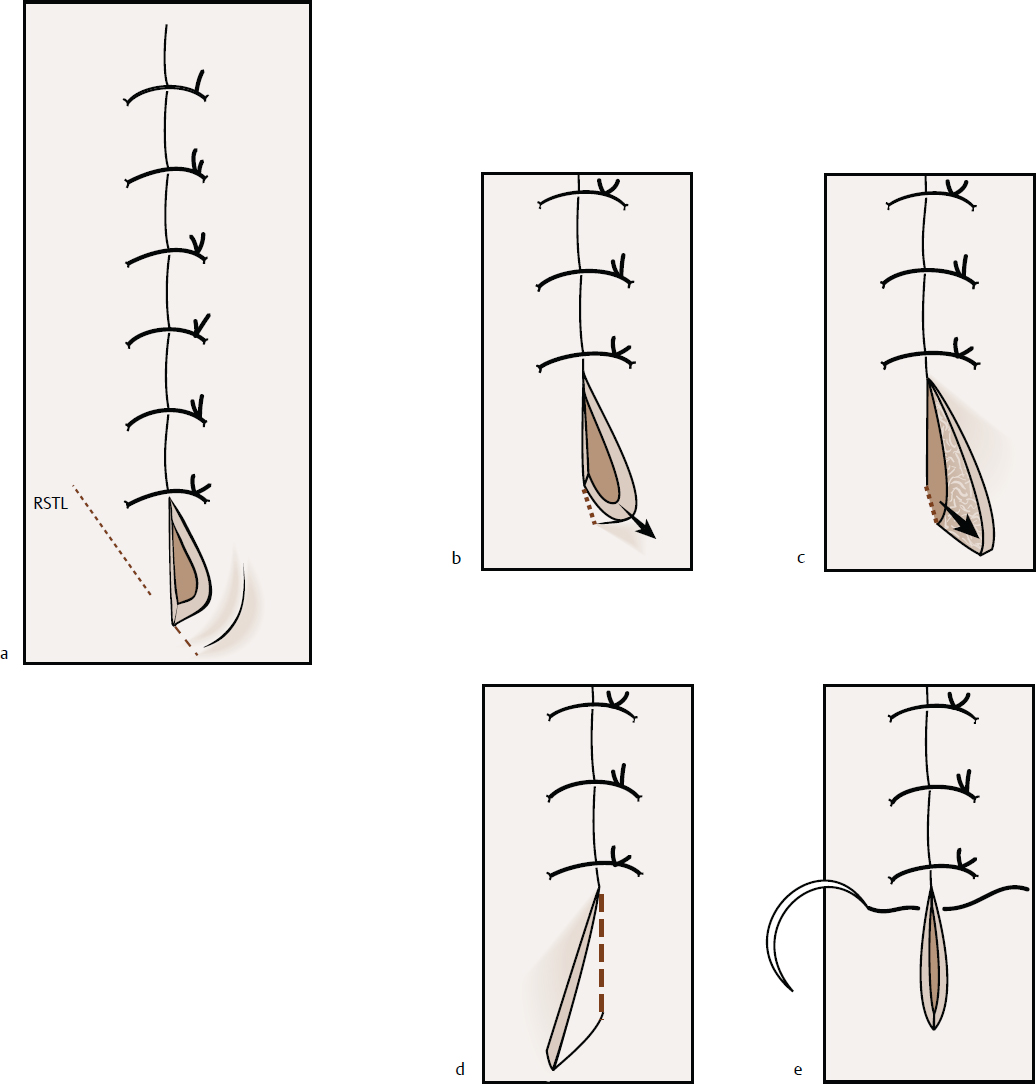
Fig. 2.3 (a–e) Correction of the “dog-ear” deformity. Abbreviation: RSTL, relaxed skin tension line.
 Wound Care
Wound Care
The suture line is typically coated with antibiotic ointment and covered with a nonadhesive gauze. Slight pressure can be obtained by taping the wound with paper or elastic tape.
Nasal wounds are treated with a rhinoplasty dressing to prevent hematoma formation and to aid in redraping of the skin–soft tissue envelope. The rhinoplasty dressing we employ is a paper tape attached with Mastisol, then cloth tape, and finally covered with an Aquaplast cast. The advantage of this dressing is that the cast is pliable at application and can be easily detached with minimal soft tissue envelope disruption by pouring Detachol directly onto the dressing.
Wound dressing can be removed in 24 to 48 hours, though nasal casts are usually removed at the time of suture removal. After dressing removal, the suture line is cleaned with hydrogen peroxide and coated with an antibiotic ointment three times per day.
Skin sutures of the face can typically be removed at day 4 to 6. Sutures of the eyelid skin can be removed at day 3 to 5, and sutures of the hair-bearing scalp at day 7 to 10. Wounds are sometimes reinforced with Mastisol and Steri-Strips for an additional week after suture removal. If the wound is under significant tension, then sutures should be left in longer, with the understanding that the likelihood of suture marks is increased.
If there is concern for hypertrophic scarring or keloid formation, then silicone gel sheeting is applied to the wound either immediately or after suture removal. Patients are instructed to use the sheeting as long as possible each day and definitely at night for 2 to 3 months. Patients are monitored in the postoperative period, and triamcinolone is injected into the scar at 4- to 6-week intervals to help prevent these untoward events.
 Defect Shape
Defect Shape
Most cutaneous defects resulting from Mohs chemosurgery are approximately circular in shape. The technique of Mohs excision also results in saucerized defects with beveled edges. The descriptions of flap designs that follow are based on a variety of defect shapes, including triangular, equilateral parallelogram, and circular. Many times the best flap design available for a given defect corresponds to a different shape than the original defect. One commonly has to remove some normal tissue and convert the defect into a larger, though more appropriately shaped, defect for proper flap closure. Flap design and drawing on the patient with a marking pen should be completed prior to removal of any normal tissue that results in a larger defect. Generally, the flaps are transferred to close the donor site, and only then is the normal tissue excised. Even if the defect shape is appropriate for the planned flap, a 1- to 2-mm edge of the wound is usually excised in a perpendicular fashion for better wound closure.
 Healing by Secondary Intention
Healing by Secondary Intention
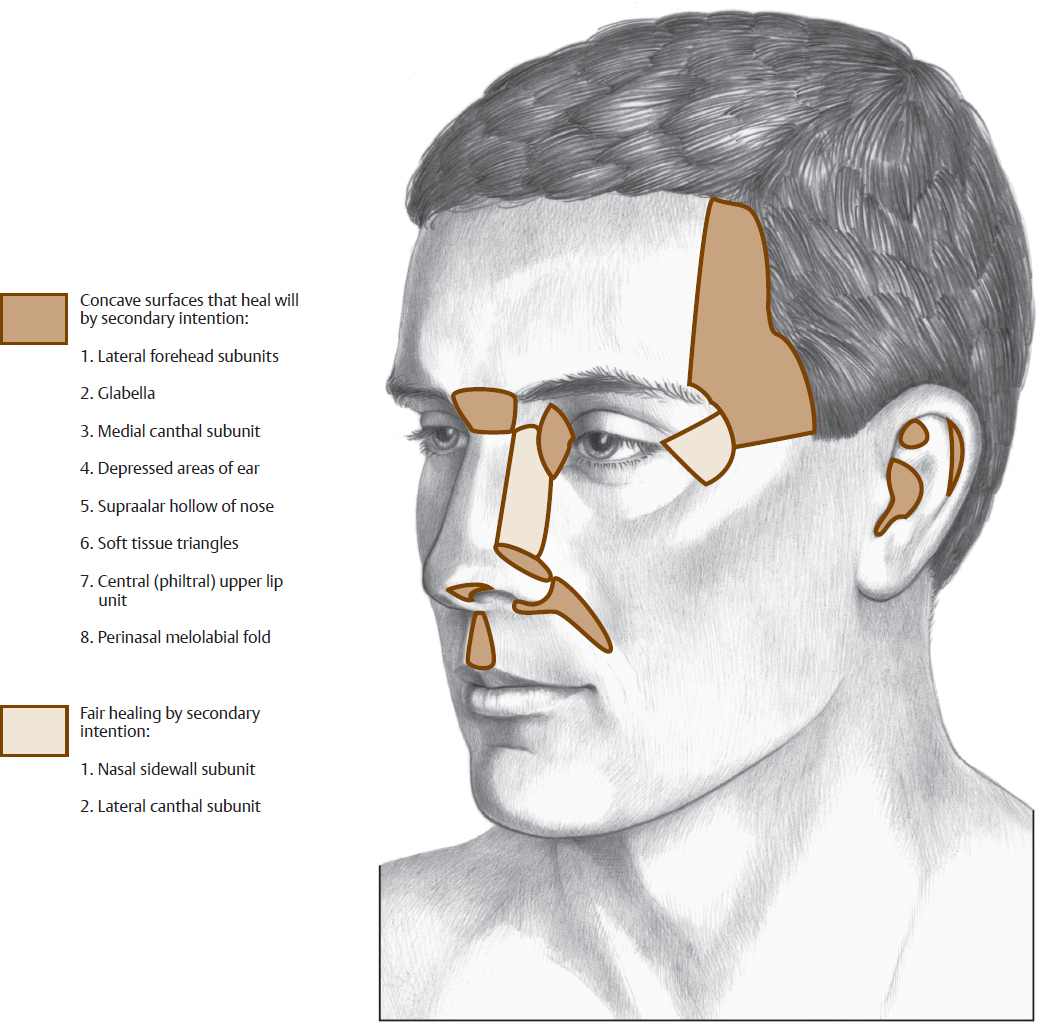
Defects in concave regions of the face heal favorably by secondary intention (Fig. 2.4). These areas include concave surfaces of the ear and nose, the temporal forehead, the glabellar region, the medial canthal subunit, the perialar/melolabial fold, and the philtral subunit of the lip. Large defects may be partially closed with local tissue advancement or “purse-string” sutures to decrease the area of the defect, thereby decreasing healing time. In areas with exposed cartilage, such as the auricle, small stab incisions or dermal punch excisions can be performed to allow granulation tissue from the opposite side of the cartilage and thus speed healing.
Healing by secondary intention requires wound care for weeks to months. The patient must be well informed and willing to accept the abnormal appearance during the healing phase. The wound is coated with antibiotic ointment and covered with a nonadherent dressing. The dressing is changed twice daily and the wound cleaned with hydrogen peroxide.
If healing by secondary intention results in an unfavorable outcome or causes distortion of local anatomical landmarks, revision surgery may then be performed. The process can be interrupted at any time and the defect repaired with a skin graft or local flap. In these cases, wound contracture will usually result in a defect that is smaller, shallower, and more easily repaired than the original.
 Skin Grafts
Skin Grafts
Split-thickness skin grafts (STSGs) are rarely used in facial reconstruction. They are generally harvested from the thigh or buttocks. A power-driven dermatome set at a thickness of 0.015 to 0.016 inch provides an adequate STSG. After harvesting the graft, the donor site is covered with a porous dressing. The graft is “pie crusted” to prevent seroma or hematoma formation.
Full-thickness skin grafts (FTSGs) are used for smaller defects (1–5 cm) and are usually harvested from head and neck sites. Color, thickness, and texture of the defect region are assessed to determine the most appropriate donor site. FTSGs are commonly harvested from the upper eyelids, the preauricular region, the postauricular region, the melolabial crease, and the supraclavicular region. When using upper eyelid skin, a blepharoplasty on the opposite eye is sometimes necessary to maintain symmetry; occasionally skin from both upper lids may be necessary for a given defect. Using a template from the defect, the proposed FTSG is marked and excised with minimal underlying subcutaneous tissue. The donor site defect is closed primarily with standing cone excised as needed.
The optimal defect bed for either an STSG or an FTSG is vascular and does not contain bare bone or cartilage. The best tissue for the bed is muscle or granulation tissue, though grafts also take well on subcutaneous tissue, perichondrium, or periosteum. If a defect contains cranial bone devoid of periosteal coverage, a local pericranial flap can be raised and used as a bed. Alternatively, drilling the bone down to the diploic space can create a vascular bed. Exposed cartilage can be treated with multiple stab incisions or dermal punch excisions to allow granulation tissue growth from the deep surface and to create a vascularized bed for grafting. A temporoparietal fascia flap can also be used to cover large areas of exposed bone or cartilage.
The FTSG is pie crusted with multiple stab incisions prior to placement. The skin graft should be further fixed to the wound bed with several placating sutures, as well as a tension-free closure at the wound edge. Once the skin graft has been sutured into place along the graft–defect margin, the site is bolstered for 3 to 5 days to prevent shearing of the graft bed surface. Cotton saturated with antibiotic ointment, nonadherent gauze (Telfa), and foam are commonly used bolster materials. Bolster sutures should be placed a few millimeters distal to the graft–defect interface to prevent cratering of the wound margins. If a seroma is noted at bolster removal, it is drained with stab incisions. Antibiotic ointment is placed on the site until healing is completed.
 Composite Grafts
Composite Grafts
Composite grafts used in local facial reconstruction usually contain skin and cartilage. The most common donor site is the ear, whereas the most common recipient sites are the nasal alar rim and columella. Composite grafts up to 1.5 cm in diameter may be used, though the risk of necrosis increases dramatically as size increases. Composites of 1 cm or less are preferred. Survival is enhanced in grafts that have contact with the donor bed on more than just the margins. For example, a graft in which only the alar margin is through and through and in which the remainder of the defect is skin only, will generally survive quite well, even with a partial-thickness area greater than 1.5 cm2. A tongue-in-groove placement, with the composite graft cartilage sandwiched between donor site skin and mucosa, will stabilize the graft and enhance survival.
No bolster is applied after the graft is inset. The graft is kept cool for 2 or 3 days postoperatively with iced saline. A short course of oral steroids is given perioperatively, and the graft is kept moist with antibiotic ointment during healing. Initially, these grafts appear pale, and over the first few days they become quite blue. Occasionally, epidermolysis and superficial skin slough occur in the first week. The graft then appears to become more pink over the ensuing weeks. These grafts should rarely, if ever, be used in patients who smoke, in radiated fields, or in other patients with any impaired vascular supply.
 Advancement Flap
Advancement Flap
An advancement flap is the simplest to design and in its most basic form involves advancing the edges of a fusiform excision together. Tension is at the wound edge and perpendicular to the incision line. Rectangular advancement flaps are used primarily in the forehead, but occasionally elsewhere (Fig. 2.5). They can be used in either a unilateral or a bilateral fashion, depending on the location of the excess tissue to be advanced. The length of each flap is generally about twice the width, although the excellent blood supply of the face will generally permit longer flaps if needed. The primary tension is at the closure of the donor site, perpendicular to the incision. When advanced, the flap width decreases slightly; therefore, the width is normally designed slightly wider than the defect size. The disparity in flap side length (shorter) and donor side length (longer) can be adjusted at closure by a combination of the principle of “halving” and Burow triangle excision, as needed. The Burow excision can be placed at one or more sites to be camouflaged in the RSTLs or at a natural anatomical boundary.
Related posts:
 Forehead
Forehead
 Scalp
Scalp
 Soft Tissue Biomechanics and Physiology
Soft Tissue Biomechanics and Physiology
 with Direct Resection of Deep Fat
with Direct Resection of Deep Fat
 value of multidetector-row CT angiography for pre-operative planning of breast reconstruction with deep inferior epigastric arterial perforator flaps
Retrospective Analysis of Never Events in Panniculectomy and Abdominoplasty Patients and Their Financial Implications
value of multidetector-row CT angiography for pre-operative planning of breast reconstruction with deep inferior epigastric arterial perforator flaps
Retrospective Analysis of Never Events in Panniculectomy and Abdominoplasty Patients and Their Financial Implications
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


