3 Scalp
Summary
This chapter focuses on the principles and anatomy that are pertinent and important with respect to reconstruction of scalp defects. Specific consideration is given to undermining and layered closure as well as the use of tissue expanders for larger defects.
Keywords: scalp, tissue expanders, rotation flap, layered closure, galea, advancement flap
The scalp is composed of five layers, recalled by the mnemonic SCALP: skin, sub cutaneous fat, galea aponeurosis, loose connective tissue, and pericranium. The galea is a strong, fibrous sheet with firm connections (via the occipitalis muscle) to the nuchal ridge posteriorly and the frontalis muscle anteriorly. The tight attachments existing between the scalp, skin and the galea significantly reduce tissue mobility in the subcutaneous planes.
Undermining in the subcutaneous plane is difficult due to extreme vascularity and it risks injury to the hair follicles. Scalp flaps are easily undermined just beneath the galea, because the space is occupied by loose connective tissue with few blood vessels. Even wide undermining at this level, however, leads to disappointingly small improvements in flap tension. Subpericranial elevation is also avascular, but it yields even less tissue laxity.
Blood supply is arranged in a radial pattern from the following five arteries: supratrochlear, supraorbital, superficial temporal, postauricular, and occipital. Abundant blood supply allows for the design of numerous small random pattern flaps. Large transposition flaps should incorporate one of the previously named arteries.
Hair emerges from the scalp at an angle. The direction in which the hair is angled varies with the scalp region. Scalp incisions should be beveled parallel to the hair follicles to preserve them (see Fig. 2.1). In areas where hair shaft direction varies, care is needed to align the incision correctly. In the pretrichal region, incisions should be beveled opposite the direction of hair follicles to allow hair regrowth through the incision.
Thick and inelastic, the scalp is resistant to such standard techniques as advancement and transposition flaps. Rotation flaps are the main reconstructive technique for scalp defects. Large defects are usually treated by tissue expansion, along with rotation or advancement flaps, as dictated by the location of the defect.
The scalp should be palpated to establish the directions of greatest mobility and the flaps designed accordingly. Scalp tissues that are closed under tension tend to stretch back up 30 to 50% of the distance closed. This problem can be reduced by using galea sutures at the time of closure.
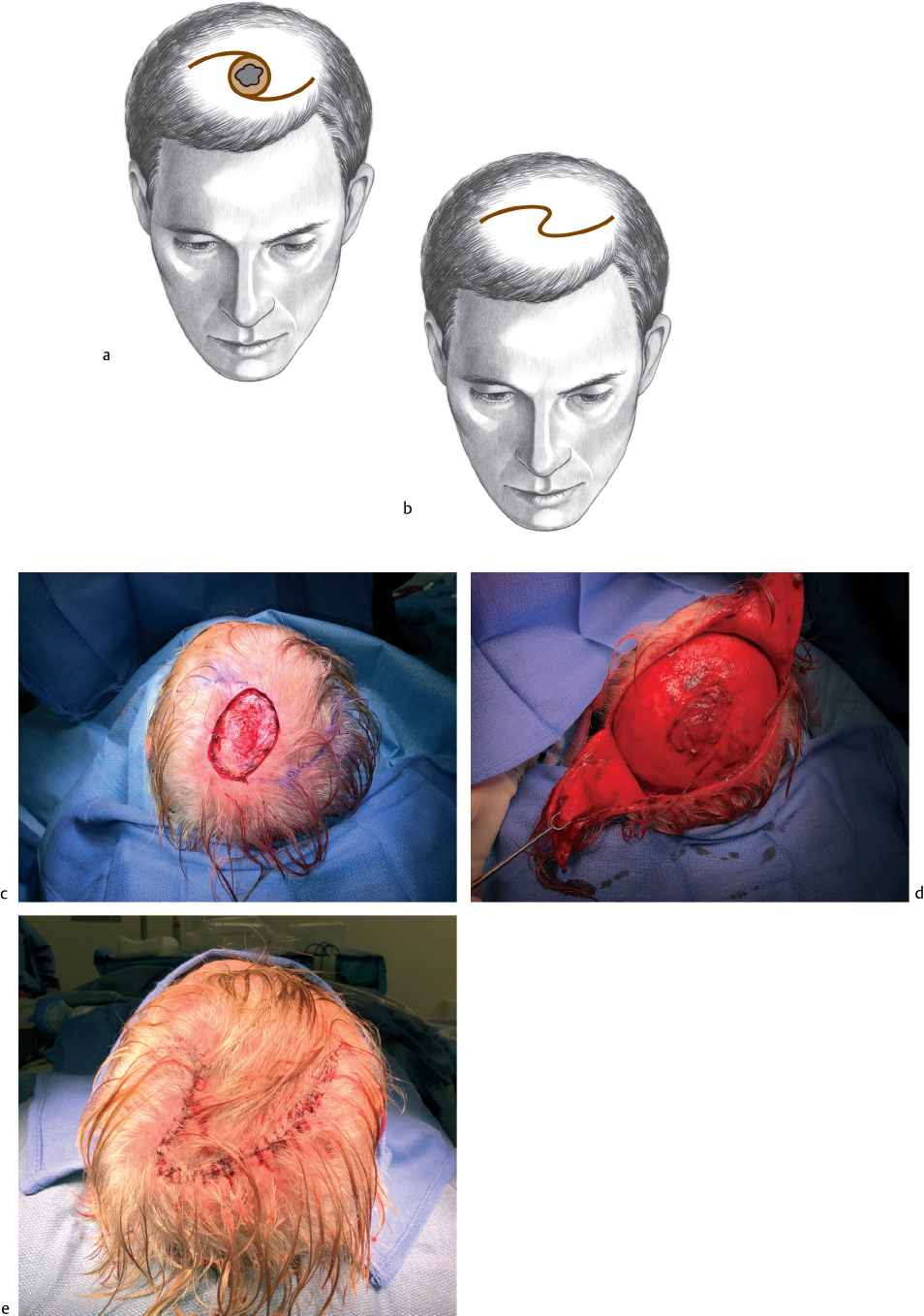
In the typical scalp, defects <3 to 5 cm in size can be closed with either unilateral or bilateral rotation flaps (Fig. 3.1). Bilateral flaps are usually selected to distribute closing tension over as much area as possible. Unilateral flaps are used primarily for defects adjacent to the hairline. The length of the sides of the rotation flap (or flaps) is typically four to six times the defect diameter to allow adequate rotation. One can design either a single or double rotation flap of maximal length, then cut back only partially to determine the actual length required (Fig. 3.2). Wide undermining in the subgaleal layer must be performed to facilitate scalp movement. Hair provides camouflage for what may seem to be inordinately long incisions for relatively small defects. The defect site is closed first. Then the long limbs are closed, using the technique of halving to distribute tension. The two limbs of the bilateral rotation flaps do not have to be equal in length, and usually are not, unless the defect is located exactly in the center of the scalp. In the situation where bilateral rotation flaps are insufficient to close a defect, one or more additional flaps may be created to convert to a “pinwheel” flap design.
Small standing cones (“dog ears”) commonly form during flap closure and will usually resolve with healing. Large standing cones can be removed using the standard Burow technique. Rotation flaps used for repair after excision of benign areas (e.g., burn scars or nevi) can be designed, incised, and rotated over the lesion prior to its removal. If necessary, a partial excision can be performed and a second stage planned.