External Mandibular Distraction for Micrognathia
Haithem M. Elhadi Babiker
DEFINITION
Distraction osteogenesis of the craniofacial skeleton was first attempted by Snyder in 1972.
In 1991, McCarthy et al. published their experience with mandibular distraction, popularizing the technique.1
Mandibular distraction osteogenesis (MDO) can be performed with either an external or internal technique. Both techniques have been proven to be successful and safe to lengthen the mandible.2
External mandibular distraction involves making a mandibular osteotomy and applying an external device to slowly and gradually lengthen the mandible. This technique is used to lengthen the hypoplastic mandible seen in multiple craniofacial conditions.
ANATOMY
The mandible is a unique U-shaped bone with two vertical rami and a horizontal body. It articulates with the skull at the temporomandibular joints and is the only movable bone of the facial skeleton.
The inferior alveolar nerve enters the mandibular foramen on the medial aspect of the ascending ramus and then extends within the mandibular body, exiting at the mental foramen.
The lingual nerve is located medial to the ramus in close proximity to the alveolar process near the third molar.
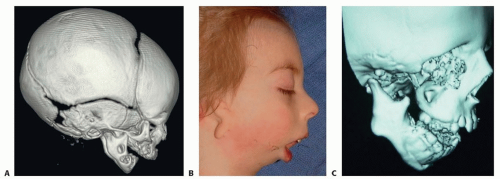
FIG 1 • A. CT scan showing the bilateral micrognathia in Pierre Robin sequence (PRS). B. Patient with hemifacial microsomia (HFM) demonstrating severe micrognathia. C. Patient with Treacher Collins syndrome (TCS) exhibiting severe micrognathia (both mandibular body and ramus), and an anterior open bite.
Patients with Pierre Robin sequence (PRS) are characterized by a hypoplastic mandibular body; the condyle and ramus are generally of normal size (FIG 1A).3
Hemifacial microsomia (HFM) is usually unilateral and is classified using a spectrum of severities from type I to type III (FIG 1B).
In Treacher Collins syndrome (TCS), the hypoplasia is similar to that seen in PRS but also includes a deep antegonial notch and downslanting mandibular body (steep occlusal plane) associated with an open bite. Some TCS mandibles may exhibit features similar to HFM (FIG 1C).4
Post-traumatic condylar fractures may also lead to mandibular hypoplasia associated with bilateral TMJ ankylosis.
PATHOGENESIS AND HISTORY
Mandibular hypoplasia occurs either as an isolated condition (possibly due to intrauterine physical growth restriction) or as part of a genetic abnormality.
Patients with mandibular hypoplasia present most commonly during the neonatal period due to obstructive sleep apnea (OSA).
HFM is the second most common craniofacial congenital anomaly, with an incidence of 1/3000 live births.
Once a child is born with mandibular micrognathia, the deformity is not progressive.
PATIENT HISTORY AND PHYSICAL FINDINGS
Patients with micrognathia usually present during infancy with tongue-based OSA, ranging from mild to very severe.2
The small mandible pushes on the tongue causing it to fall back and obstruct the airway.
Mild cases present with noisy breathing during sleep.
More severe cases present with apneic episodes, cyanotic spells, and feeding abnormalities.5
The child expends most of his or her energy trying to breathe, and hence has no energy to feed.
Poor weight gain and failure to thrive are strong indicators of severe OSA.6
Neonates with severe OSA require urgent admission to the neonatal intensive care unit (NICU) for airway stabilization.
Treatment modalities include prone positioning, nasopharyngeal airway, tongue-lip adhesion, and in very severe cases, tracheostomy.
The main objective of mandibular distraction is to avoid a tracheostomy or to achieve decannulation in patients with a tracheostomy.
IMAGING
Lateral cephalometric radiographs can be used to identify the mandibular micrognathia. In neonates, a lateral skull x-ray at a distance of 72 in. is used to evaluate the hypoplastic mandible.
The best imaging modality is a three-dimensional computed tomography (3D CT) scan to characterize the mandible and to render a volumetric measurement of the airway.
Low-dose CT scans use very low radiation (comparable to traditional radiographs) without compromising image quality (FIG 2).
DIFFERENTIAL DIAGNOSIS
HFM, 1:3000 live births
PRS, 1:14 0007
TCS, 1:50 000 live births8
Nager syndrome
Post-traumatic condylar fractures
Stickler syndrome, velocardiofacial syndrome, fetal alcohol syndrome, trisomy 21 and 22, and Kabuki syndrome9
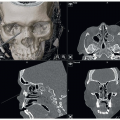
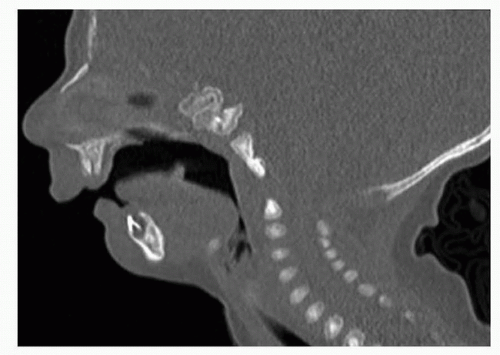 FIG 2 • CT scan showing mandibular micrognathia, retropositioning of the tongue, and narrow airway stripe. |
NONOPERATIVE MANAGEMENT
Prone and lateral decubitus positioning.
Nasopharyngeal airway, oxygen support, and possible tongue suture.10
ICU care and close monitoring is critical to prevent rapid deterioration.
A multidisciplinary team comprised of neonatology, otolaryngology, pulmonology, plastic surgery, and genetics should make the decision regarding treatment planning.
The infant is evaluated with a polysomnography and a microlaryngoscopy/bronchoscopy, which examines the entire airway and differentiates lower airway from upper airway problems.
Mild cases are treated with conservative measures.
SURGICAL MANAGEMENT
Mandibular distraction is generally undertaken during the neonatal period.
The main objective of the operation is to lengthen the mandible, which pulls the tongue forward to relieve the tonguebased respiratory obstruction.
The main steps of the surgery are as follows:
Intraoral incision(s) to expose the posterior aspect of the mandible.
Saw or bur to make a corticotomy in the ascending ramus/angle of the mandible.
Self-drilling pins into the mandible proximal and distal to the corticotomy site.
If a rigid external distraction (RED) device is used, place the anterior mandibular plate and secure it to the mandible with monocortical screws.
Use a 5-mm osteotome to convert the corticotomy into an osteotomy to completely liberate the mandibular segments.
Attach the distraction device to the pins.
If an RED is used, attach the halo component to the anterior mandibular plate using 25-gauge wire.
Close the intraoral wound in watertight fashion.
Wait 1 to 3 days (latency period) and then activate the device (activation period) until the desired final position of the mandible is achieved.
Maintain the device in position until the new bone mineralizes (consolidation period).
Remove the distraction device at the end of the consolidation period.
The operation is performed bilaterally in cases of PRS, TCS, and Nager syndrome; or unilaterally in cases of HFM.
Selection criteria for mandibular distraction include severe mandibular micrognathia (maxillomandibular differential of greater than 8 mm), polysomnogram showing severe OSA, and difficulty with breathing and feeding.8
Preoperative Planning
A 3D CT scan is obtained to delineate the morphology of the mandible, the position of the inferior alveolar nerve and the teeth follicles.
Cephalometric measurements can be obtained from the CT scan to quantify the mandibular hypoplasia.
Positioning
The patient is positioned supine.
The procedure is generally performed in conjunction with ENT and pulmonology to perform the MLB and assist with intubation.
The procedure is done under general anesthesia.
The patient is intubated nasally; the endotracheal tube is sutured to the nasal septum and secured appropriately to the forehead (FIG 3).
A foam donut stabilizes the head.
Approach
Surgery is performed through an intraoral approach with percutaneous placement of the pins.
 FIG 3 • Endotracheal tube secured to the forehead and sutured to the nasal septum. |
TECHNIQUES
▪ External Mandibular Distraction With Pins
Exposure and Dissection
Inject local anesthetic with vasoconstrictor to infiltrate the area of dissection in the posterior mandible.
Insert a bite block/gauze sponge on the opposite side of dissection to adequately open the mouth.
Expose the area of dissection by placing two Langenbeck retractors to pull away the cheek.
In very small babies, malleable retractors can be used instead. Place a tongue retractor to protect the tongue.
A 3-cm incision is made in the area of the ascending ramus and angle of the mandible.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree