Key points
- •
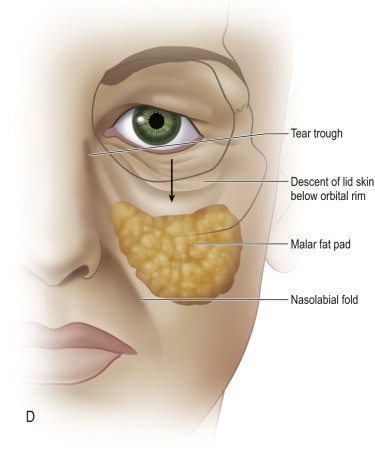
Descent of the midfacial structures and volume deflation lead to characteristic aging changes, including infraorbital concavity, a defined lower lid–cheek junction and nasolabial line formation.
- •
Complete release of the malar soft tissue complex allows its elevation and suspension, thereby restoring volume and convexity to the infraorbital region.
- •
Lateral canthal fixation and correction of horizontal lid laxity are essential to prevent complications of lid malposition and scleral show.
- •
A direct and secure fascia-to-fascia suturing of the midface complex is necessary to maintain its newly elevated positioning.
- •
The potential for periocular complications with both functional and aesthetic consequences necessitates familiarity with reconstructive oculoplastic procedures that may be needed for correction, including canthoplasty and spacer grafts.
Introduction
In the realm of facial rejuvenation, there has been a relatively recent appreciation of the changes that occur over time in the malar region. A combination of malar fat pad ptosis, facial volume loss and actinic skin changes inevitably lead to the stigmata of midface aging, including descent of the lid–cheek junction, formation of the nasojugal groove and nasolabial fold development. In response to this, surgeons have developed various techniques of central facial release and resuspension to address these changes and create an overall more natural and harmonious result following facial aesthetic surgery. While most techniques emphasize vertical elevation of midfacial soft tissue, critical analysis of both results and complications has led to numerous refinements over the years including the extent of subperiosteal undermining, inclusion of lateral canthal fixation, lateral flap suspension sutures, development of endoscopic vs open techniques, and lately, the role of autogenous fat transfer.
The earliest techniques for midfacial rejuvenation utilized temporal and preauricular incisions with extensive peripheral to central dissection. In contradistinction, the transblepharoplasty subperiosteal technique can be done effectively through a single subciliary incision to address the midface, with other incisions added in those cases of more significant aging that require simultaneous browlift or necklift procedures. By confining dissection to the central subperiosteal plane, there is less risk of facial nerve injury and less interruption of blood supply to facial soft tissues. The subperiosteal dissection allows a more complete release of midfacial soft tissues including the retaining ligaments. The composite flap of malar fat, SMAS, muscle and periosteum can then be most effectively elevated to reposition cheek skin, restore malar prominence, eliminate tear trough deformities, and soften nasolabial lines.
Indications
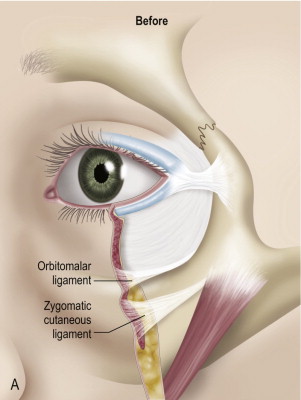
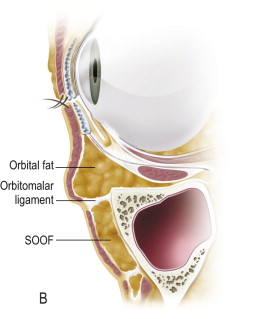
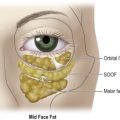
The youthful eyelid lacks lower lid laxity and skin excess. It is characterized by a positive canthal tilt, a lower lid level just superior to the inferior limbus, and a smooth convexity from the lid to the cheek region at the level of the infraorbital rim. As aging occurs, the lid loses some of its tone and the skin, muscle and fat descend over the relatively fixed orbitomalar, zygomatic and nasolabial retaining ligaments. These locations of these ligaments are shown in Figure 9.1 . Additionally, volume loss in the face has a deflationary effect which leads to loss of underlying support and further exacerbation of midface descent.
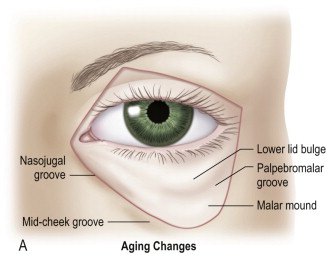
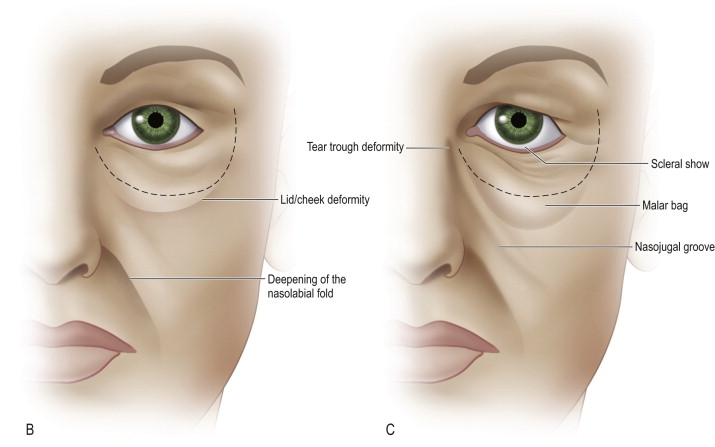
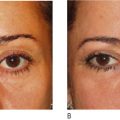
These anatomic changes manifest in the central face in several ways ( Figure 9.2 ). As tarsoligamentous laxity increases, the eye assumes a more rounded shape with a negative canthal tilt as the lateral commissure descends. Malar fat pad ptosis causes loss of cheek prominence and a lengthening of the lid–cheek junction. Nasojugal groove formation occurs creating a ‘tired’ appearance. With attenuated skin now occupying the infraorbital region, the infraorbital rim and the lower lid fat pads become more visible through the skin. The nasolabial fold deepens as cheek soft tissue descends over the nasolabial retaining ligament. There may even be some descent of the lateral oral commissure with increased laxity of the upper lip elevators.
Elevation and resuspension of the lower eyelid skin and cheek fat pads combined with lateral canthal fixation counteract midface descent and re-establish lower lid tone. By eliminating the nasojugal groove, decreasing prominence of the infraorbital fat pads, and diminishing the nasolabials, a midface lift can successfully and safely restore a natural, youthful appearance to the eyes.
Patient selection
Patients with the aforementioned anatomic changes are considered appropriate midface lift candidates. A comprehensive evaluation of the entire face including the brows, mandibular line and anterior neck is essential to determine if additional procedures may be beneficial in creating overall facial rejuvenation and harmony. In those patients with co-existent aging changes, for optimal results, the cheeklift can be combined with an endoscopic browlift and rhytidectomy.
Pre-operative assessment should include a history of ocular health, including the presence of dry eyes, previous ophthalmologic procedures such as LASIK, and use of anticoagulants including aspirin. Inflammatory conditions such as blepharitis can be exacerbated by surgery and are therefore best treated prior to elective surgery. Patients prone to dry eyes, such as those with tear dysfunction syndromes or post-LASIK therapy, need to be aware of the fact that there is often a transient worsening of this symptom following surgery. They should be examined for adequate eye protective mechanisms and educated about the need for ocular lubricants in the weeks following surgery.
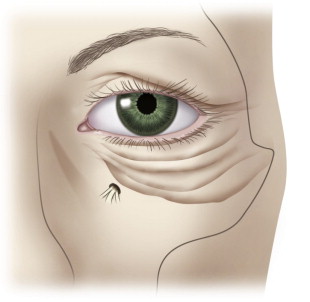
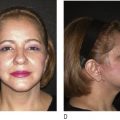
In examining the midface, it is necessary to assess the degree of vertical tissue descent in determining the proper surgical procedure. Lesser degrees of descent may necessitate only a lower lid blepharoplasty, whereas more defined changes including infraorbital hollowing and prominence of the lid–cheek margin respond more effectively to a cheeklift procedure. The degree of fat herniation should be assessed; while occasionally resection may be required, more often this fat can be redraped over the infraorbital rim to create a smooth transition from the lid to the cheek. Malar festoons are characterized as lateral outpouchings of skin located along the malar bone, such as those rendered in Figure 9.3 . These are usually incompletely addressed by standard lower lid bleharoplasty and respond more completely to subperiosteal dissection and soft tissue redraping. The tear trough region should be assessed to determine pre-operatively if free fat transfer should be done as an adjunct to the midface elevation. Skin quality should be evaluated as the presence of static rhytids or hyperpigmentation may guide the surgeon to perform simultaneous laser resurfacing or chemical peels.
The lower lid itself should also be examined for laxity. A pre-operative snap back test and measuring intraoperative lid distraction are useful indicators of lower lid tone. This information can then be used to determine if a canthopexy vs a canthoplasty would be most beneficial in restoring lower lid support and preventing post-operative complications related to lid malposition. Similarly, the degree of eye prominence should also be noted prior to surgery, as this can influence optimal placement of the canthal anchoring suture. In particular, patients with very prominent eyes are at risk for scleral show, and should be considered for supraplacement of the lateral canthal suture and possibly even a spacer graft for additional lower lid support.
Pre-operative preparation
The procedure is done under general anesthesia. With the patient in the supine position and head positioned in a gel or foam circular headrest, markings are made. The arc of the subciliary marking is extended 10–12 mm lateral to the lateral canthus in one of the natural transverse creases. Corneal protectors are placed over the globes and the areas of planned incisions and dissection infiltrated with 0.5% lidocaine with epinephrine.
Technique
The subciliary incision is made through the skin and carried out to the lateral extension. In this lateral region, electrocautery is used to carry this incision through the orbicularis muscle to the periosteum overlying the lateral orbital rim. A pocket is created superiorly and laterally over the lateral orbital rim to adequately expose the periosteum and the deep temporal fascia superiorly.
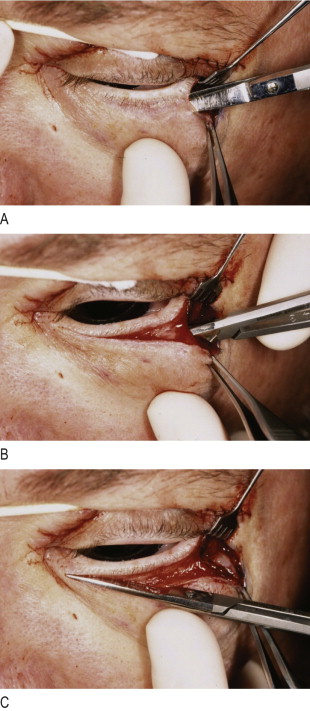
Turning attention to the skin incision beneath the lashes, the orbicularis muscle is divided 4 mm below the inferior edge of the tarsus, thereby preserving the inferior arcade. Intraoperative photos of this are shown in Figure 9.4 . Cautery is used to elevate a skin–muscle flap at the pre-septal plane. This dissection is carried out over the malar area with release of the arcus marginalis. Proceeding inferiorly, the orbitomalar ligament is divided at its insertions to the periosteum just below the inferior orbital rim and extending out laterally to the level of the lateral canthus. Cautery is now used to incise the periosteum just below the edge of the infraorbital rim. Subperiosteal dissection can now proceed using either a periosteal elevator or the electrocautery. Medially, this dissection will extend to the nasomaxillary suture line with care taken to preserve the infraorbital nerve.
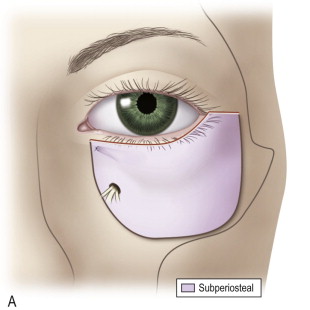
Inferiorly, dissection will be to the inferior edge of the malar bone and and laterally to the zygomaticomaxillary suture line, avoiding dissection over the zygomatic arch. The extent of subperiosteal dissection is shown in Figure 9.5 . The zygomaticofacial nerve as depicted in Figure 9.6 will be sacrificed over the lateral portion of the malar eminence to allow full mobilization of the midface. There is only minimal resultant sensory loss to the overlying skin with this maneuver. Once the subperiosteal pocket has been created, the periosteum along the periphery is released using either the cautery, reverse periosteal elevator or finger. Because all dissection has been subperiosteal, potential injury to branches of the facial nerve is minimized. The malar soft tissue complex has now been freed posteriorly from its bony attachments, allowing vertical elevation and fixation. This maneuver will ultimately redrape the superior border of the malar fat pad and SOOF over the inferior and inferolateral orbital rim to elevate the lid–cheek junction and restore fullness to the infraorbital region.
Related posts:
 Anatomy of the upper and lower eyelids
Anatomy of the upper and lower eyelids
 Correction of the tear trough deformity with hyaluronic acid
Correction of the tear trough deformity with hyaluronic acid
 Orbital aging and harmony in orbital rejuvenation
Orbital aging and harmony in orbital rejuvenation
 Midface elevation: one single suture
Midface elevation: one single suture
 Alloplastic augmentation to improve blepharoplasty and midfacial results
Alloplastic augmentation to improve blepharoplasty and midfacial results
 Is the transpalpebral approach to the upper and midface rejuvenation a safe method?
Is the transpalpebral approach to the upper and midface rejuvenation a safe method?
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


