| Blind, painful eye |
| Intractable endophthalmitis or corneal ulceration with no visual potential |
| Anterior ruptured globe with no visual potential |
| Significant phthisis bulbi with contracture of the sclera |
| Panophthalmitis with infection of posterior sclera |
| History of necrotizing scleritis |
| Known intraocular malignancy or inability to rule out occult intraocular malignancy |
| History of prior eye diseases, trauma, or surgeries |
| Prior medical management for blind painful eyes or endophthalmitis |
| Overall medical health and surgical risk profile |
| Psychological status of patient (particularly for younger patients) |
| Complete examination of both the surgical eye AND the fellow eye to evaluate for visual potential, pathology, and occult malignancies (including ophthalmic ultrasound and/or CT or MRI imaging if fundoscopic examination is limited) |
| Pupillary response (reverse testing if globe and pupil are degenerated) |
| Motility |
| Eyelid and superior sulcus |
| Conjunctiva and fornices |
| Orbit (volume) |
| Intraocular pressure |
Introduction
Evisceration surgery is performed in end-stage blind, painful eyes or infected eyes for which medical management has failed and there is no visual potential. The surgery involves removing the intraocular contents entirely and oftentimes the cornea and portions of the anterior sclera as well.
During the preoperative evaluation, it is critical to perform a complete dilated exam on both eyes. Visual potential and any concomitant ocular pathology should be evaluated fully. In cases of trauma, structural integrity of the injured eye should be evaluated to determine if any useful vision could be regained. In cases where the posterior pole cannot be adequately examined on fundoscopy, ophthalmic ultrasound, with or without CT or MRI imaging, should be performed to rule out occult intraocular tumors. Patients are strongly advised to wear protective eyewear at all times to preserve the fellow eye.
The decision between evisceration and enucleation ( Chapter 73 ) varies by surgeon. With cases of known or suspected intraocular malignancy, enucleation is the standard of care, not only to avoid seeding the intraocular malignancy into the orbit but also to allow for complete pathologic examination with implications toward prognosis and treatment.
One of the main advantages of evisceration surgery is that there is less disruption of the orbital structures, such as the extraocular muscles, optic nerve, and orbital fat. This often results in improved cosmesis, ocular motility, and orbital volume preservation. Moreover, evisceration surgery is faster and can be more comfortably performed with a retrobulbar block if the patient is not a good surgical candidate due to medical co-morbidities. Additionally, in the case of endophthalmitis from a perforated corneal ulcer, the infected intraocular tissues are less likely to spill deep into the orbit causing a potential implant infection, orbital cellulitis, or meningitis.
The main disadvantages of evisceration surgery are the risks of sympathetic ophthalmia and occult malignancy. Unlike in enucleation surgery, in which the total intraocular contents are removed, it is impossible to remove all the pigmented uveal melanocytes during evisceration since some will inevitably remain in the emissary channels of the sclera. With the advent of modern immunomodulatory medications, sympathetic ophthalmia can be more effectively treated than in the past, but remains an important and serious condition that deserves discussion during the preoperative evaluation. As such, some ophthalmologists feel that an extensive history of intraocular surgeries and/or ocular traumas is a relative contraindication to evisceration.
Occult intraocular malignancy is another important risk with evisceration. Trauma or intraocular pathology often causes media opacities that prevent a detailed fundoscopic examination of the eye in question. In these cases, evaluation by ophthalmic ultrasonography and/or CT or MRI imaging is advisable to rule out any readily apparent tumors. Nonetheless, diffuse choroidal melanomas are characterized by minimal choroidal thickening and can be missed on echography. If there is any concern or doubt about the presence of an intraocular malignancy, enucleation should be favored over evisceration.
Restoring orbital volume after evisceration is essential to achieving optimal aesthetic and functional outcomes. A multitude of different orbital implants have been described over the past 50 years. As compared to enucleation surgery, there is relative orbital volume preservation with evisceration due to preservation of the sclera and optic nerve and minimal trauma-induced atrophy to surrounding orbital tissues.
The volume of the implant placed is limited by the size of the sclera and whether the corneal button and any surrounding sclera are removed during the operation. Typically, a size 14- or 16-mm spherical implant can be placed. In order to place a larger implant in the socket to prevent a superior sulcus deformity, a posterior scleral window can be created. This allows a larger implant to be placed such that its posterior portion extends deep into the orbit through the scleral window. With this modification, an 18-, a 20-, or even a 22-mm spherical implant can be placed. When available, our preference is to use a 20-mm conical implant (equivalent in volume to a 22-mm spherical implant) when possible, as this allows the tapered end of the implant to project beyond the posterior sclera in the same cone-shaped configuration as the orbit.
Complications related to evisceration include superior sulcus deformity, upper eyelid ptosis, and lower eyelid malpositions. Socket contracture is a surgical condition that is challenging to treat, and meticulous surgical technique at the time of evisceration can help prevent this condition.
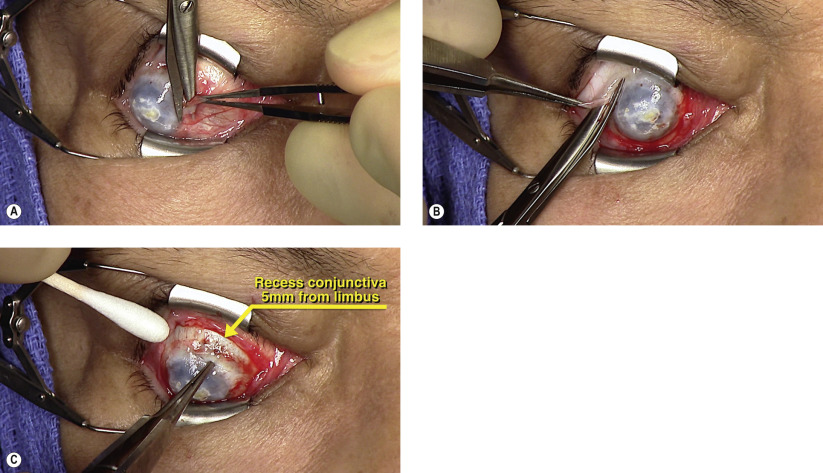
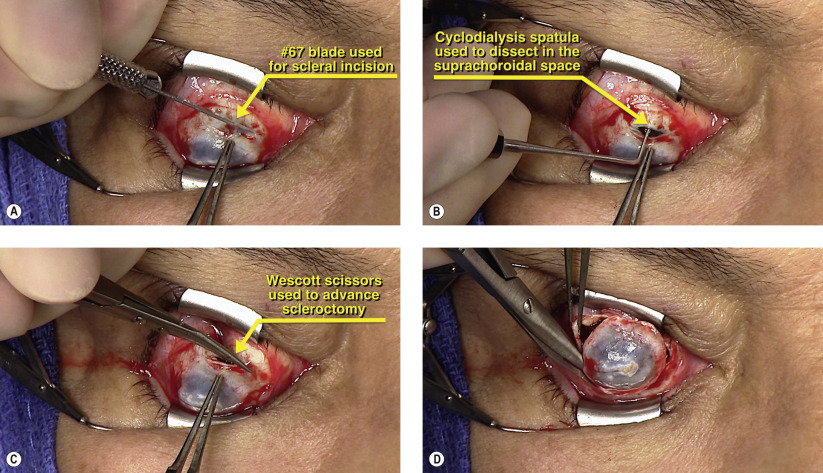
Surgical Technique
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


