This chapter provides images of a collection of conditions that result from errors in metabolism. Many of these diseases manifest in the skin secondary to the deposition of material such as amyloid, porphyrin, calcium, lipid, and urate crystals.
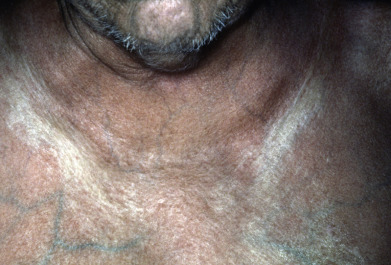
Amyloidosis includes systemic and localized cutaneous forms. Systemic amyloidosis is characterized clinically by scattered shiny, firm papules, plaques, and nodules; macroglossia; and, most commonly, easy bruising with the typical “pinched purpura.” Cutaneous amyloidosis includes the keratinocyte-derived amyloid deposited in macular and lichenoid patterns, as well as the nodular, plasma cell-derived form.
Porphyrins are required to build heme, but when specific enzyme defects cause them to accumulate, they can cause tissue damage after being activated by visible light (400-410 nm). This interaction with light explains why porphyrias are conditions that demonstrate photosensitivity with vesicles, bullae, and erosions in the typical photodistributed pattern on the face, upper chest, and dorsal hands and forearms. Other clinical findings of note in porphyrias include hyperpigmentation, skin fragility, and hypertrichosis.
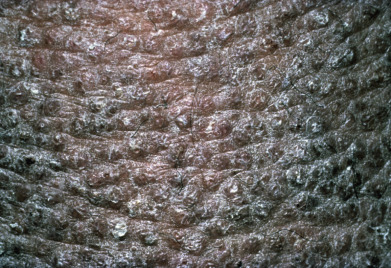
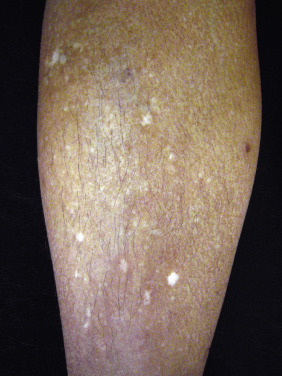
Calcinosis cutis has been categorized into dystrophic, metastatic, and iatrogenic, depending on the cause. All forms present with rock-hard papules, nodules, or plaques that can extrude whitish chalky material. Patient history, full physical examination, and laboratory investigations will help distinguish between these forms of calcinosis. Idiopathic calcinosis cutis also occurs in specific locations, such as the scrotum, where it often does not require further clinical workup.
Deposition of lipid in the skin leads to yellow- or orange-colored papules, plaques, or masses that are categorized clinically based on their anatomic location and morphology. These include tuberous and tendinous xanthomas that often occur over joints requiring differentiation from gout. Eruptive xanthomas present with widespread papules, whereas plane xanthomas are characterized by larger yellowish patches. Other more localized xanthomas include palmar xanthomas on the hands and xanthelasma palpebrarum on the eyelids. Although xanthelasmas can be found in the setting of normal lipid levels, all patients with xanthomas require a workup to confirm the diagnosis and screen for a wide range of hyperlipidemias.
This portion of the atlas includes the previously mentioned deposition-related conditions, the cutaneous manifestations of diabetes mellitus, and rarer syndromes, including lipoid proteinosis and Fabry disease (angiokeratoma corporis diffusum).



























Related posts:
 Atopic Dermatitis, Eczema, and Noninfectious Immunodeficiency Disorders
Atopic Dermatitis, Eczema, and Noninfectious Immunodeficiency Disorders
 Seborrheic Dermatitis, Psoriasis, Recalcitrant Palmoplantar Eruptions, Pustular Dermatitis, and Erythroderma
Seborrheic Dermatitis, Psoriasis, Recalcitrant Palmoplantar Eruptions, Pustular Dermatitis, and Erythroderma
 Bacterial Infections
Bacterial Infections
 Chronic Blistering Dermatoses
Chronic Blistering Dermatoses
 Melanocytic Nevi and Neoplasms
Melanocytic Nevi and Neoplasms
 Genodermatoses and Congenital Anomalies
Genodermatoses and Congenital Anomalies
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


