Abstract
Neoplasms of the epidermis ( Table 5.1 ) are derived from a proliferation of basal cells or keratinocytes. Epidermal growths are recognized clinically by a localized thickening of the epidermis that often is accompanied by thickening of the stratum corneum, which is called hyperkeratosis or scale . Large, indurated, rapidly growing, crusted, or ulcerated tumors suggest a malignant process and should undergo biopsy. Unless injured or irritated, benign growths do not bleed or become crusted or ulcerated.
Actinic Keratosis
- 1.
Precancerous
- 2.
Prevent with sun protection
Definition
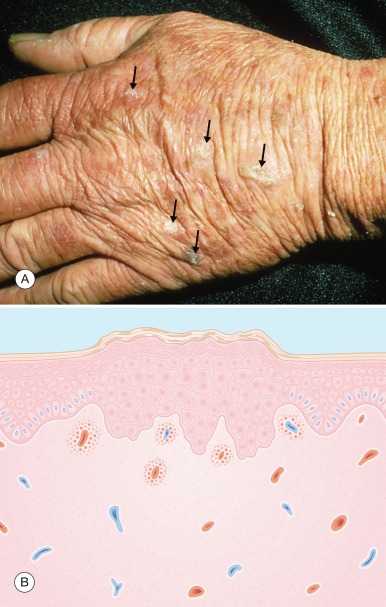
Actinic (solar) keratosis is a precancerous neoplasm of the epidermis caused by the ultraviolet (UV) portion of sunlight. The abnormal keratinocytes in actinic keratoses are confined to the epidermis and constitute a premalignant change. The proliferation of these abnormal cells is clinically manifest as a rough, scaling patch or papule ( Fig. 5.1 ).
Although considered premalignant, most actinic keratoses do not progress to skin cancer.
| Frequency (%) a | Etiology | Physical Examination | Differential Diagnosis | Laboratory Test (Biopsy) | |
|---|---|---|---|---|---|
| Actinic keratosis | 1.7 | Sunlight | Ill-marginated, reddish, rough, scaling patch or papule | Squamous cell carcinoma Seborrheic keratosis Superficial basal cell carcinoma Lichenoid keratosis | When thick scale or indurated base |
| Basal cell carcinoma | 1.7 | Sunlight | Yes | ||
| Nodular | Pearly nodule with telangiectasia, often has central depression or ulcer | Molluscum contagiosum Squamous cell carcinoma Sebaceous hyperplasia Nevus Merkel cell carcinoma Trichoepithelioma | |||
| Pigmented | Blue-black plaque or nodule with pearly border | Malignant melanoma Nevus Seborrheic keratosis | |||
| Superficial | Red, scaling, crusted eczematous appearing patch | Psoriasis Eczema Bowen’s disease Lichenoid keratosis | |||
| Sclerosing | Whitish, slightly depressed, sometimes crusted pink plaque/patch | Squamous cell carcinoma Non-healing scar | |||
| Corn | 0.4 | Friction | Hyperkeratotic papule or nodule with compact clear core | Wart | No |
| Molluscum contagiosum | 0.3 | Poxvirus | Translucent papule with umbilicated center | Comedo Nodular basal cell carcinoma | No |
| Seborrheic keratosis | 1.6 | – | Tan-brown, greasy, pasted-on papule or plaque | Wart Actinic keratosis Nevus Malignant melanoma Pigmented basal cell carcinoma | No |
| Skin tag | 0.5 | – | Soft, skin-colored, pedunculated papule | Neurofibroma nevus | No |
| Squamous cell carcinoma | 0.2 | Sunlight Viruses Chemicals | Flesh-colored, hard, crusted or scaling nodule, often ulcerated | Keratoacanthoma Basal cell carcinoma Wart Lichenoid keratosis Actinic keratosis Merkel cell carcinoma Trichoepithelioma Nevus sebaceous | Yes |
| Wart | 5.2 | Papillomavirus | No | ||
| Common | Flesh-colored, scaling, vegetative papule or nodule, skin lines interrupted, studded with black puncta | Corn Squamous cell carcinoma | |||
| Flat | Reddish, smooth, flat, well-demarcated papule | Lichen planus Comedo Corn | |||
| Plantar | Solitary, grouped or mosaic scaling papules, skin lines interrupted, studded with black puncta | Squamous cell carcinoma | |||
| Genital | Soft, moist, cauliflower-appearing papules or nodule | Squamous cell carcinoma Secondary syphilis | No |
a Percentage of new dermatology patients with this diagnosis seen in the Hershey Medical Center Dermatology Clinic, Hershey, PA.
Incidence
The incidence of actinic keratoses varies with (1) skin pigmentation; (2) geographic location; and (3) amount of sun exposure. Thus, the incidence of actinic keratoses is high in Caucasians who have light skin, live in the southern United States where there is an abundance of natural sunlight, and engage in frequent outdoor activity. In the authors’ clinic, 1.7% of new patients were seen because of actinic keratoses, although the incidence would be higher in the “Sunbelt.” Moreover, in many patients, actinic keratoses are an incidental finding.
Light skin and abundant sun exposure may result in actinic keratoses.
History
Risk factors can usually be elicited in the history. The patient may have a genetic predisposition. Fair-skinned Caucasians have the least amount of protective pigment. A family history of skin cancer or an Irish or Anglo-Saxon heritage is frequently obtained. Second, the geographic location where the patient has lived directly influences the amount of UV light exposure. As one moves toward the equator, the UV light intensity increases dramatically. Last, the occupational and recreational activities of the patient with reference to sun exposure provide another clue. Farmers, sailors, and others with occupations that require working outdoors have a high amount of UV light exposure. Similarly, persons who spend many hours at the poolside or on the beach are at higher risk.
Physical examination
Actinic keratoses are 1 to 10 mm, reddish, ill-marginated patches and papules that have a rough, yellowish brown, adherent scale. Their ill-defined margins make them indistinct to the casual observer. Their rough-textured surface is often easier to feel than to see. Actinic keratoses occur in sun-exposed areas: the face, dorsum of the hands and forearms, neck, upper back, chest, and lower legs. They generally are found on UV-damaged skin that has a yellowish hue, wrinkles, and freckled pigmentation.
An actinic keratosis is rough, scaling, and ill marginated; it is often easier felt than seen.
Differential diagnosis
An actinic keratosis must be differentiated from other epidermal tumors. Most often, it is confused with a seborrheic keratosis . The well-demarcated, “pasted on” appearance of a seborrheic keratosis differentiates it from an actinic keratosis. In situ squamous cell carcinoma is a larger plaque with margins that are well defined, in contrast to the margins of an actinic keratosis. Hypertrophic or indurated actinic keratosis ( Fig. 5.1 ) cannot be differentiated with certainty from squamous cell carcinoma and should undergo biopsy. Superficial basal cell carcinoma , which resembles is situ squamous cell carcinoma clinically, is occasionally confused with actinic keratosis. Lichenoid keratosis should also be considered in the differential diagnosis. A lichenoid keratosis is an inflamed lentigo or thin seborrheic keratosis which is well-demarcated with some residual tan/brown coloration within the pink inflamed lesion.
- ●
Seborrheic keratosis
- ●
Squamous cell carcinoma
- ●
Superficial basal cell carcinoma
- ●
Lichenoid keratosis
Laboratory and biopsy
Actinic keratosis is characterized histologically by a partial-thickness dysplasia of the epidermis ( Fig. 5.1B ). A hyperkeratosis with underlying irregular hyperplasia of mildly dysplastic keratinocytes is seen. A chronic inflammatory response is present in the dermis. All thick and indurated actinic keratoses should undergo biopsy to rule out squamous cell carcinoma, as well as lesions that have not responded to previous treatment.
Indurated and therapeutically unresponsive actinic keratoses should undergo biopsy to rule out carcinoma.
Therapy
Prevention by reducing sunlight exposure is the most effective form of therapy. Patients who are sensitive to the sun or have developed actinic keratoses should wear protective clothing such as broad-brimmed hats and long-sleeved shirts when outside. Sunscreens with a sun protective factor (SPF) of 30 should be used on exposed skin. The regular use of sunscreens prevents the development of new actinic keratoses, as well as hastening the resolution of those that already exist. Avoidance of sun exposure at midday (from 10:00 a.m. to 2:00 p.m.), when UV radiant energy is most intense, is recommended. Patient awareness and education should begin in childhood.
Use sun protection to prevent more actinic damage.
Cryosurgery with liquid nitrogen is the most common treatment for actinic keratoses and is most useful when a few lesions are present. Thick, hypertrophic, actinic keratoses are also better treated in this way. Freezing can be accomplished in a manner similar to that described for warts.
Avoid overzealous treatment of thin actinic keratoses because of possible scarring.
Topical chemotherapy with 5-fluorouracil cream 5% (Efudex) is the most common means of treating multiple actinic keratoses. 5-Fluorouracil inhibits DNA synthesis by blocking the enzyme thymidylate synthase. When 5-fluorouracil is applied to normal skin, little reaction occurs, but when it is applied to sun-damaged skin, those areas with actinic keratoses become inflamed. The medication is applied to the involved areas twice daily. Erythema develops within several days. Subsequently, within 2 to 4 weeks, the actinic keratoses become painful, crusted, and eroded, at which time the medication is stopped. Patients need to be warned about the discomfort and cosmetically unsightly effects of 5-fluorouracil, which are temporary and resolve after discontinuing treatment. Because of the marked amount of inflammation that can occur, small regions may be treated at a time in patients with extensive actinic keratoses. A few patients may become allergic to 5-fluorouracil. Patients with severe actinic damage can be expected to require treatment every couple of years. Alternative agents include (1) diclofenac gel 3% (Solaraze), a nonsteroidal antiinflammatory drug (NSAID), applied twice daily for 3 months; (2) imiquimod cream 5% (Aldara), a topical immune response modifier, applied twice weekly for 4 months; (3) ingenol mebutate 0.015% gel applied daily to the face/scalp for 3 days and 0.05% gel applied daily to the extremities/trunk for 2 days respectively; and (4) photodynamic therapy, chemical peel, or laser.
Prevention
- ●
Sunscreen ≥ SPF 30
- ●
Broad-brimmed hat, long-sleeved shirt, and pants
- ●
Avoidance of intense midday sun (from 10:00 a.m. to 2:00 p.m.)
Initial
- ●
Cryotherapy with liquid nitrogen
Alternative
- ●
5-Fluorouracil 5% cream twice daily for 2–3 weeks
- ●
Diclofenac 3% gel twice daily for 3 months
- ●
Imiquimod 5% cream twice weekly for 16 weeks
- ●
Ingenol mebutate 0.015% or 0.05% gel applied daily to the face or extremities/trunk for 3 or 2 days, respectively
- ●
Photodynamic therapy, chemical peel, or laser
Course and complications
In patients with chronically sun-damaged skin, the acquisition of more actinic keratoses can be expected. Some actinic keratoses spontaneously disappear (up to 26%), although others may develop into squamous cell carcinoma. The number that do develop into squamous cell carcinoma appears to be small, less than 1 in 1000 within 1 year. Metastases from squamous cell carcinomas arising in actinic keratoses are very uncommon.
Actinic keratosis has a small potential of developing into a squamous cell carcinoma.
Pathogenesis
Actinic keratoses are produced by UV radiation-induced damage to keratinocyte DNA. This results in unrepaired or error-prone repaired DNA. Abnormal replication occurs and results in epidermal cellular hyperplasia. The cells within an actinic keratosis are arranged in a disorderly way and have increased mitoses and an abnormal chromatin pattern. Other precancerous keratinocytic neoplasms similar to actinic keratoses are caused by artificial UV light, X-irradiation, or polycyclic aromatic hydrocarbons.
Basal Cell Carcinoma
- 1.
Malignancy of the epidermal basal cell
- 2.
Very rarely metastasizes
- 3.
Different types have different appearances
Definition
Basal cell carcinoma is a malignant neoplasm arising from the basal cells of the epidermis. Although these cancers rarely metastasize, their potential for local destruction attests to their malignant nature. UV radiation is the cause of most basal cell carcinomas in humans. Four clinically and histopathologically distinct types of basal cell carcinoma are recognized: nodular, pigmented, superficial, and scarring (sclerotic).
Incidence
Basal cell carcinoma is the most common human malignant disease; it affects more than 2 million persons annually in the United States. Of the new patients in the authors’ clinic 2% are seen for basal cell carcinoma. The increased frequency in adult Caucasians is related to sun exposure.
Basal cell carcinoma is the most common skin cancer, but it very rarely metastasizes.
History
The patient with basal cell carcinoma seeks medical attention because of a new growth, especially if it is a nonhealing, easily bleeding lesion. There may be a personal or family history of skin cancer. The risk of basal cell carcinoma is higher in patients with light skin, in those who live in southern latitudes, and in those who work or play outdoors. Frequently, these patients have a history of sunburning easily and tanning poorly.
Physical Examination
The usual patient with basal cell carcinoma has fair skin, blue eyes, blonde or red hair, and actinic-damaged skin manifested by freckles, yellow wrinkling, and actinic keratoses. Basal cell carcinoma occurs in sun-exposed skin, particularly the head and neck.
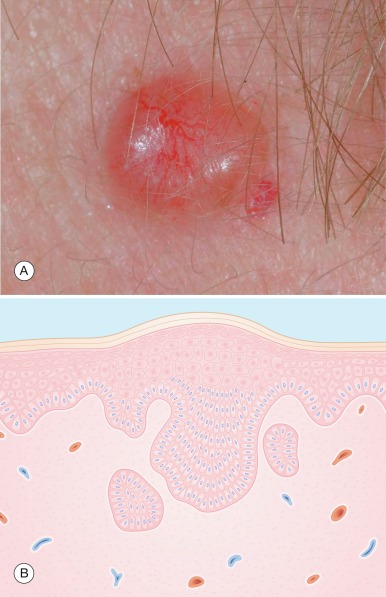
A “pearly” appearance is the most characteristic feature of a nodular basal cell carcinoma.
The nodular type ( Fig. 5.2 ) of basal cell carcinoma is the most common. It is a “pearly,” semi-translucent papule or nodule that often has a central depression or crater, telangiectasia, and a rolled, waxy border. Ulceration and crusting can occur. Nodular basal cell carcinoma occurs most frequently on the face, especially the nose.
Types of basal cell carcinoma:
- 1.
Nodular
- 2.
Pigmented
- 3.
Superficial
- 4.
Scarring (sclerotic)

Pigmented basal cell carcinoma ( Fig. 5.3 ) is a shiny, blue–black papule, nodule, or plaque. The pigment is often speckled, and a pearly, rolled margin can be seen when the tumor is viewed from the side.

Superficial basal cell carcinoma ( Fig. 5.4 ) occurs most frequently on the thorax. It is a red, slightly scaling, well-demarcated, eczematous appearing patch. Centrally, it may become slightly eroded and crusted, subsequently leaving an atrophic, slightly depressed center. Its shape is oval to round, with a characteristic thread-like, pearly, rolled border. It is often referred to as multicentric superficial basal cell carcinoma because it skips islands of normal skin, similar to the way a forest fire may surround a stand of trees yet leave it unburned.

The scarring (sclerotic or morpheaform) basal cell carcinoma ( Fig. 5.5 ) is an atrophic, white, slightly eroded, or crusted plaque that often looks like a scar. It is frequently depressed and is the least common and most aggressive type of basal cell carcinoma.

Differential Diagnosis
Nodular basal cell carcinoma and sebaceous hyperplasia are sometimes difficult to differentiate clinically. Sebaceous hyperplasia is the proliferation of sebaceous glands surrounding a hair follicle that appears as a 1- to 3-mm, yellowish papule with overlying telangiectasia and a central pore. The yellowish coloration and central pore help to differentiate it from a basal cell carcinoma. Other epithelial growths that resemble a nodular basal cell carcinoma include a nonpigmented nevus , molluscum contagiosum , Merkel cell carcinoma, trichoepithelioma, fibrous papule of the nose, lichenoid keratosis, and squamous cell carcinoma .
Pigmented basal cell carcinoma can be confused with a seborrheic keratosis , pigmented nevus , and, most importantly, malignant melanoma . The pearly, rolled border of pigmented basal cell carcinoma helps to differentiate it from a malignant melanoma. If doubt exists, an excisional or deep shave biopsy should be performed.
Superficial basal cell carcinoma resembles a patch of dermatitis . It can be confused with psoriasis , nummular dermatitis , and squamous cell carcinoma . A persistent solitary lesion and lack of response to topical steroids clinically differentiate superficial basal cell carcinoma from dermatitis or psoriasis. A skin biopsy is the only way to differentiate it from squamous cell carcinoma in situ .
Any nonhealing scar-like lesions should undergo biopsy to rule out a scarring basal cell carcinoma.
Nodular
- ●
Sebaceous hyperplasia
- ●
Flesh-colored nevus
- ●
Molluscum contagiosum
- ●
Merkel cell carcinoma
- ●
Trichoepithelioma
- ●
Fibrous papule of the nose
- ●
Squamous cell carcinoma
- ●
Pigmented
- ●
Seborrheic keratosis
- ●
Pigmented nevus
- ●
Malignant melanoma
- ●
Superficial
- ●
Dermatitis
- ●
Lichenoid keratosis
- ●
Squamous cell carcinoma
- ●
Scarring
- ●
Scar
- ●
Laboratory and Biopsy
The diagnosis of basal cell carcinoma should be confirmed by a shave or punch biopsy. The technique of skin biopsy is reviewed in Chapter 4 . The tumors are made up of uniform cells that resemble the basal layers of the epidermis (see Fig. 5.2B ). They have a uniform, large, oval, blue nucleus with indistinct cytoplasm. The tumor extends from the epidermis into the dermis as nodular or cystic structures, bands, or strands, or as buds from the epidermis. The nodular areas have peripheral palisading with retraction from the surrounding stroma. The cells in some basal cell carcinomas have a “squamoid” appearance, which makes them difficult to differentiate from squamous cell carcinoma. The infiltrative, morpheaform, micronodular, and mixed histologic subtypes of primary basal cell carcinoma are more aggressive and more difficult to eradicate.
A chronic eczematous patch or nonhealing crusted lesion should be biopsied to rule out a superficial basal cell carcinoma.
Therapy
Treatment of basal cell carcinoma should be individualized according to the location of the lesion, the histopathologic type, the age of the patient, the general health of the patient, the size of the basal cell carcinoma, and whether it is primary or recurrent. Recurrence of basal cell carcinoma is related particularly to location on the nose or ear, size more than 2 cm, and histologic pattern of micronodular, infiltrative, and morpheic types. Treatment modalities include scalpel excision, curettage and electrodesiccation, radiotherapy, cryotherapy, and topical 5-fluorouracil or imiquimod. Each treatment must be properly selected to achieve a high cure rate. Surgical modalities are those most frequently used and have the best cure rates. The surgical techniques are reviewed in Chapter 4 .
Excision with primary suture closure, the most frequently used form of therapy, allows for histologic assessment of surgical margins. When the wound is large, grafts or tissue transposition flaps may be used to achieve closure. Excision is good for most basal cell carcinomas, but is the treatment of choice for large basal cell carcinomas, recurrent tumors, sclerosing types of basal cell carcinoma, basal cell carcinomas at sites of high recurrence such as the nose or ear, and basal cell carcinoma that extends into the subcutaneous tissue. A specialized form of excision using detailed mapping of the extent of the tumor with histologic orientation is the Mohs micrographic surgical technique . This meticulous procedure is most often used for basal cell carcinomas on the head and neck, recurrent basal cell carcinoma, and primary tumors with a high risk of recurrence.
Mohs micrographic surgery has the highest cure rate and preserves the most normal skin. It is indicated for most facial/neck basal cell carcinomas and for recurrent basal cell carcinomas.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


