| Blind and painful eye |
| Sympathetic ophthalmia prophylaxis after uveal prolapse |
| Intraocular malignancy (e.g. choroidal melanoma, retinoblastoma) |
| Phthisis bulbi with disfigurement and blind eye from multiple causes (post-traumatic, retinal detachment, end-stage glaucoma, endophthalmitis) |
| Vision potential of eye |
| Pupillary response (reverse testing if globe and pupil are degenerated) |
| Motility |
| Eyelid and superior sulcus |
| Conjunctiva and fornices |
| Orbit (volume) |
| Intraocular pressure |
| Complete examination of fellow eye |
| Timing of injury |
| Oncologic work-up for cases of intraocular malignancy |
| Psychological status of patient (particularly for younger patients) |
Introduction
Enucleation is one of the oldest ophthalmic procedures and involves removal of the entire globe and portions of the optic nerve. The indications include blind and painful eye from a variety of causes, intraocular malignancy, and sympathetic ophthalmia prophylaxis after severe ocular trauma.
Importantly, the loss of an eye – especially a seeing eye – is strongly associated with depression and other psychological disturbances and, accordingly, referral to mental health professionals is often indicated.
During the evaluation, a careful examination is performed of the eye to be enucleated. The visual potential should be fully assessed, particularly in traumatic cases where some usable vision may remain. In cases where no view of the posterior pole is possible, a B-scan ultrasound should be performed to rule out occult intraocular tumor. The fellow eye must also be carefully evaluated and any pathology treated as the patient will be monocular. Patients are strongly advised to wear protective eyewear at all times to preserve the fellow eye.
The preference for evisceration ( Chapter 72 ) or enucleation varies between surgeons. With cases of known or suspected intraocular malignancy, enucleation is the standard of care, as complete pathologic examination is necessary. Obtaining a long optic nerve segment is particularly important in the management of retinoblastoma as this malignancy can spread via the optic nerve. Furthermore, a systemic oncologic evaluation should be performed in cases of intraocular malignancy.
Restoring orbital volume after enucleation is paramount to achieving the best aesthetic and functional outcomes. A multitude of different orbital implants have been described over the past 50 years. The generally accepted consensus is to place the largest possible implant at the time of surgery. Currently used alloplastic implant materials at the time of writing include porous polyethylene (Medpor, Stryker Surgical, Kalamazoo, MI), hydroxyapatite (Bio-Eye, IOI, San Diego, CA) silicone, acrylic, and aluminum oxide bioceramic (FCI, Cedex, France).
Fibrovascular integration of orbital implants lessens the chance of implant extrusion. Implants may also be wrapped with tissue such as fascia, autologous or donor sclera or bovine pericardium to decrease the risk of extrusion and to facilitate attachment of the extraocular muscles. The newer implants such as porous polyethylene do not require wrapping and the extraocular muscles can be directly attached to the implant.
Pegging of the implant can be performed to improve motility of the prosthetic but the high complication rates with this modification have largely limited its widespread use. Other complications related to enucleation include superior sulcus deformity, upper eyelid ptosis, and lower eyelid malpositions. Socket contracture is a challenging surgical condition and meticulous surgical technique at the time of enucleation can minimize this problematic condition.
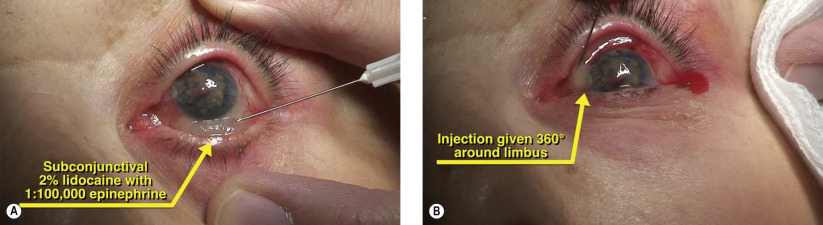
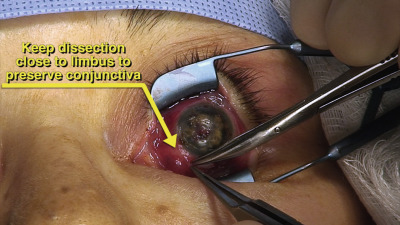
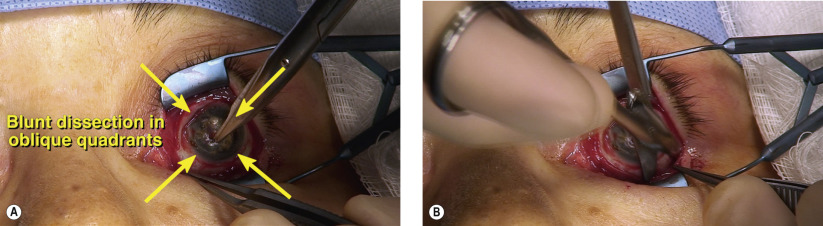
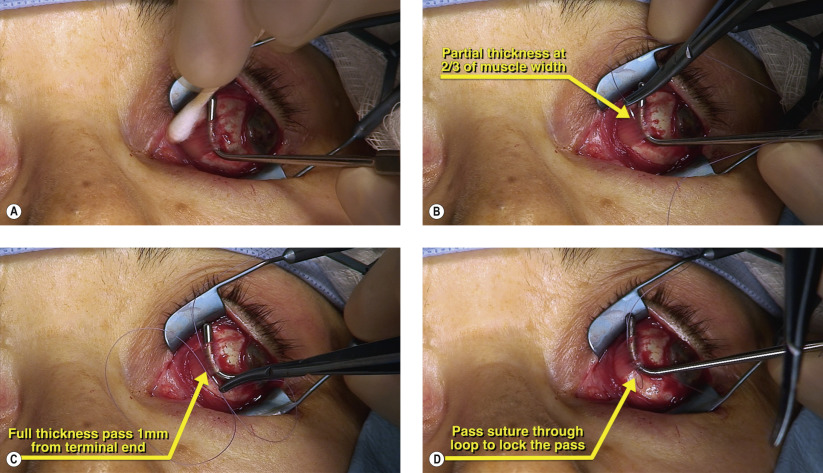
Surgical Technique
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


