The Enhanced Recovery After Surgery (ERAS) protocol is a multidisciplinary, multimodal, and evidence-based approach to perioperative management. The ERAS pathway has been applied to numerous major surgical procedures throughout various specialties and has shown reduced postoperative morbidity, reduced opioid use, higher patient satisfaction, and shortened hospital length of stay. In the current health care climate, there has been a growing focus on optimizing the quality of care for patients and reducing the overall cost burden of health care. In this article, the authors review the ERAS pathways for breast reconstruction procedures and discuss the outcomes of implementation of these pathways.
Key points
- •
The Enhanced Recovery After Surgery (ERAS) protocol is a multidisciplinary, multimodal, and evidence-based approach to perioperative management.
- •
ERAS protocols help to streamline perioperative care based on evidence-based review and consensus across all multidisciplinary aspects of care in breast reconstruction.
- •
In plastic surgery procedures, ERAS pathways have been shown to reduce hospital length of stay and opioid consumption, which may have cost-saving implications down the line. They also enhance the patient experience by improving postoperative analgesia, nausea, and vomiting.
Background
The Enhanced Recovery After Surgery (ERAS) protocol is a multidisciplinary, multimodal, and evidence-based approach to perioperative management. This concept was first introduced in 1997 by a group of general surgeons from Europe, led by Henrik Kehlet, , with a background experience in colorectal “fast-track surgery.” A formal research group, called the ERAS Study Group, was then formed by a group of surgeons from several academic hospitals in Europe in 2001, with the aim of exploring an improved care pathway for patients undergoing open colorectal procedures, with the specific goals of improving care, reducing cost, and reducing length of hospital stay. The ERAS pathway has since been applied to numerous major surgical procedures throughout various specialties and has shown very promising results, namely reduced postoperative morbidity, reduced opioid use, and shortened hospital length of stay. , , The ERAS Society was subsequently established in 2003 with the aim of further developing formal perioperative care pathways to improve recovery through evidence-based practices.
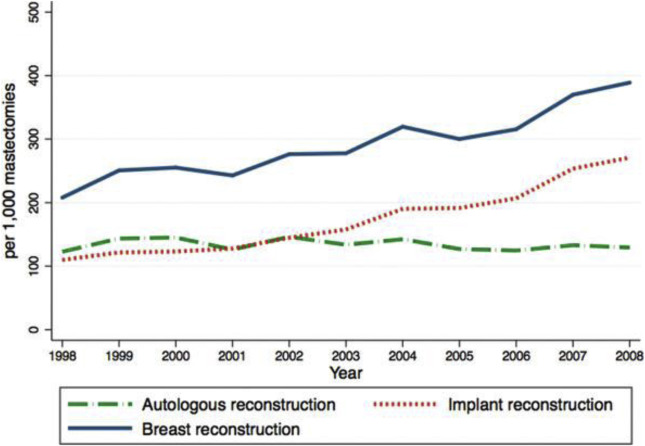
Breast cancer is the most common malignancy in women worldwide according to the World Health Organization, contributing more than 25% to new cancer diagnoses in 2012 (excluding nonmelanoma skin cancer). In the United States, there has been a gradual increase in immediate and delayed reconstruction over the past few decades ( Fig. 1 ). In 2017, there were 106,000 breast reconstructions in the United States, which represents a 35% increase from 2000.
In the current health care climate, there has been a growing focus on optimizing the quality of care for patients and reducing the overall cost burden of health care. More attention has thus been given to ERAS pathways as a quality improvement initiative in breast reconstruction. Several studies have examined the efficacy and safety of ERAS pathways in patients undergoing breast reconstruction. In this article, the authors review the ERAS pathways for breast reconstruction procedures.
Enhanced Recovery After Surgery Society recommendations in breast reconstruction
In 2017, a consensus report developed by the ERAS Society provides guidelines specific for breast reconstruction ( Table 1 ). These guidelines describe 18 care elements in the preoperative, intraoperative, and postoperative periods for breast reconstruction. These care elements will be reviewed based on the following consensus data :
- 1.
Preadmission information, education, counseling
- 2.
Preadmission optimization
- 3.
Perforator flap planning
- 4.
Perioperative fasting
- 5.
Preoperative carbohydrate loading
- 6.
Venous thromboembolism prophylaxis
- 7.
Antimicrobial prophylaxis
- 8.
Postoperative nausea and vomiting prophylaxis
- 9.
Perioperative and intraoperative analgesia
- 10.
Standard anesthetic protocol
- 11.
Preventing intraoperative hypothermia
- 12.
Perioperative intravenous fluid management
- 13.
Postoperative analgesia
- 14.
Early feeding
- 15.
Postoperative flap monitoring
- 16.
Postoperative wound management
- 17.
Early mobilization
- 18.
Postdischarge home support and physiotherapy
| Item | Recommendation | Evidence Level | Recommendation Grade |
|---|---|---|---|
| Patients should receive detailed preoperative counseling | Moderate | Strong |
| For daily smokers, 1 mo of abstinence before surgery is beneficial. For patients who are obese, weight reduction to achieve a BMI ≤30 kg/m 2 before surgery is beneficial. For alcohol abusers, 1 mo of abstinence before surgery is beneficial. For appropriate groups, referral should be made to resources for these behavior changes | Moderate (smoking) | Strong |
| High (obesity) | Strong | ||
| Low (alcohol) | Strong | ||
| If preoperative perforator mapping is required, CTA is recommended | Moderate | Strong |
| Preoperative fasting should be minimized, and patients should be allowed to drink clear fluids up to 2 h before surgery | Moderate | Strong |
| Preoperative maltodextrin-based drinks should be given to patients 2 h before surgery | Low | Strong |
| Patients should be assessed for venous thromboembolism risk. Unless contraindicated, and balanced by the risk of bleeding, patients at a higher risk should receive low-molecular-weight heparin or unfractionated heparin until ambulatory or discharged. Mechanical methods should be added | Moderate | Strong |
| Chlorhexidine skin preparation should be performed, and intravenous antibiotics covering common skin organisms should be given within 1 h of incision | Moderate | Strong |
| Women should receive preoperative and intraoperative medications to mitigate postoperative nausea and vomiting | Moderate | Strong |
| Women should receive multimodal analgesia to mitigate pain | Moderate | Strong |
| General anesthesia with TIVA is recommended | Moderate | Strong |
| Preoperative and intraoperative measures, such as forced air, to prevent hypothermia should be instituted. Temperature monitoring is required to ensure the patient’s body temperature is maintained higher than 36°C | Moderate | Strong |
| Overresuscitation or underresuscitation of fluids should be avoided, and water and electrolyte balance should be maintained. Goal-directed therapy is a useful method of achieving these goals. Balanced crystalloid solutions, rather than saline, are recommended. Vasopressors are recommended to support fluid management and do not negatively affect free flaps | Moderate | Strong |
| Multimodel postoperative pain management regimens are opioid sparing and should be used | High | Strong |
| Patients should be encouraged to take fluids and food orally as soon as possible, preferably within 24 h after surgery | Moderate | Strong |
| Flap monitoring within the first 72 h should occur frequently. Clinical evaluation is sufficient for monitoring, with implantable Doppler devices recommended in cases of buried flaps | Moderate | Strong |
| For incisional closure, conventional sutures are recommended. Complex wounds following skin necrosis are treatable with debridement and negative-pressure wound therapy | High (sutures), moderate (NPWT) | Strong |
| Patients should be mobilized within the first 24 h after surgery | Moderate | Strong |
| Early physiotherapy, supervised exercise programs, and other supportive care initiatives should be instituted after discharge | Moderate | Strong |
Preadmission Information, Education, and Counseling
Recommendation
Patients should receive detailed preoperative counseling.
Discussion of the surgical and anesthetic plans with the patient helps manage their expectations and concerns about the procedure. Offering patients preoperative education enables them to be a part of the decision-making process about breast reconstruction. This discussion has been shown to reduce anxiety and improve patient satisfaction independent of the reconstruction type. ,
Preadmission Optimization
Recommendation
For daily smokers, 1 month of abstinence before surgery is beneficial.
For patients who are obese, weight reduction to achieve a body mass index less than or equal to 30 kg/m 2 before surgery is beneficial. For alcohol abusers, 1 month of abstinence before surgery is beneficial. For appropriate groups, referral should be made to resources for these behavior changes.
Variables, such as smoking, alcohol consumption, poor nutrition, diabetes, and obesity, are some factors that are known to have an adverse effect on postoperative outcomes in breast reconstruction surgery. Patients with an active smoking history have more mastectomy flap necrosis, reconstructive failure, and higher rates of infection compared with nonsmokers. , Heavy alcohol consumption (defined as 5 or more drinks on each of 5 or more days in the past 30 days) has also been shown to increase the risk of surgical site infections. It is therefore recommended that patients stop smoking and drinking alcohol for at least 1 month before surgery.
Obesity (>30 kg/m 2 ) is associated with flap loss and donor-site morbidity as well as increases the risk of surgical site infection and venous thromboembolism. Patients are encouraged to lose weight before surgery. In obese patients, muscle-preserving flaps (ie, deep inferior epigastric perforator [(DIEP] flap) reduce the risk abdominal wall complications, such as hernia, compared with non-muscle-sparing flaps (ie, free or pedicled transverse rectus abdominis musculocutaneous [TRAM] flap). ,
With respect to diabetes, the National Surgical Quality Improvement Program (NSQIP) data on 29,736 women with breast reconstruction showed an increased risk of overall surgical complications (Operating room, 1.85). Poor glycemic control is associated with worse outcomes in primary closure of surgical wounds in these high-risk patients. Although not formally included in the consensus report, it has been shown that glucose levels greater than 200 mg/dL are associated with worse outcomes in terms of wound healing. Current guidelines outlined by the Society for Healthcare Epidemiology of America recommend maintaining postoperative blood glucose of 180 mg/dL or lower.
Perforator Flap Planning
Recommendation
If preoperative perforator mapping is required, computed tomographic angiography (CTA) is recommended.
Despite risks of contrast allergy, nephrotoxicity, and exposure to radiation, modern CTA scanning protocols have been able to reduce the amount of radiation patients are exposed to. Prior metaanalysis has shown the benefits of CTA with respect to reducing operative time, postoperative flap-related complications, and donor-site morbidity compared with Doppler ultrasonography.
Preoperative Fasting
Recommendation
Preoperative fasting should be minimized, and patients should be allowed to drink clear fluids up to 2 hours before surgery.
A 2003 Cochrane Review of 22 randomized controlled trials showed that drinking clear fluids 2 hours before surgery is safe and does not increase the risk regurgitation and aspiration. The ERAS guidelines for gastrointestinal surgery recommend a 6-hour preoperative fasting for solid foods and 2-hour fasting for clear liquids before general anesthesia. The guidelines note that the recommendations have not been applied to patients at increased risk of gastric emptying.
Preoperative Carbohydrate Loading
Recommendation
Preoperative maltodextrin-based drinks should be given to patients 2 hours before surgery.
Studies have shown that maltodextrin-based drinks (400 mL) taken 2 hours before surgery have positive metabolic effects, such as increasing insulin sensitivity and reducing preoperative thirst and anxiety. The effect of carbohydrate loading preoperatively reduces the catabolic effects of surgery, including loss of nitrogen and protein, lean body mass, and muscle strength, resulting in a reduced length of hospital stay. Furthermore, for patients with well-controlled type 2 diabetes, a carbohydrate drink given up to 3 hours before surgery (instead of 2 hours) along with their normal medication does not delay gastric emptying and allows glucose concentrations to return to baseline.
Prophylaxis Against Venous Thromboembolism
Recommendation
Patients should be assessed for venous thromboembolism risk. Unless contraindicated, and balanced by risk of bleeding, patients at higher risk should receive low-molecular-weight heparin or unfractionated heparin until they are ambulatory or discharged. Mechanical methods (as with intermittent pneumatic compression) should be added.
Patients undergoing breast reconstruction procedures are at greater risk for venous thromboembolism. NSQIP data on 68,285 patients have shown an almost 2-fold increased risk of venous thromboembolism compared with lumpectomy or mastectomy alone (0.41% vs 0.13% and 0.29%, respectively; P <.0001). According to the American Society of Plastic Surgeons Executive Committee–approved Caprini Risk Assessment Module, patients undergoing immediate reconstruction after mastectomy meet criteria for “higher” risk of venous thromboembolism and are “highest” risk if they are obese or elderly. , For this population, pharmacologic anticoagulation with or without mechanical methods (ie, intermittent pneumatic compression) is recommended. , The ERAS guidelines recommend that prophylaxis be initiated before surgery and continue for at least 7 to 10 days. Although low-molecular-weight heparin has been shown not to increase bleeding risk in some studies, , other studies have shown low-molecular-weight heparin may have a higher bleeding risk than unfractionated heparin in breast surgery procedures. ,
Antimicrobial Prophylaxis
Recommendation
Chlorhexidine skin preparation and intravenous antibiotics covering common skin organisms should be given within 1 hour of incision.
The risk of infection following mastectomy is higher than other clean surgeries (3%–15% vs 2%). , This risk is further increased with the addition of a flap or prosthesis. Prophylactic antibiotics have been shown to decrease the risk of surgical-site infections. Antibiotics against common skin organisms (ie, cephalosporins) should be administered 1 hour before incision. , Despite the common practice of continued use of postoperative antibiotics while surgical drains are in place, prolonged use of antibiotics in breast reconstruction beyond 24 hours has not been proven beneficial in implant- and flap-based surgeries. , Chlorhexidine-based antiseptic skin preparations applied before surgery have been shown to decrease surgical site infections. ,
Preoperative and Intraoperative Prophylaxis Against Postoperative Nausea and Vomiting
Recommendation
Women should receive preoperative and intraoperative multimodal medications to mitigate postoperative nausea and vomiting.
Metaanalysis has demonstrated the efficacy of 5-hydroxytryptamine-3 receptor antagonists over placebo in reducing postoperative nausea and vomiting in breast surgery. Steroids alone have been shown to reduce postoperative nausea, vomiting, and pain. When combined, steroids and 5-hydroxytryptamine-3 receptor antagonists have superior effects than either alone. Preoperative neurokinin-1 receptor antagonists provide even further reduction in postoperative nausea and vomiting compared with 5-hydroxytryptamine-3 receptor antagonists.
Preoperative and Intraoperative Analgesia
Recommendation
Women should receive multimodal analgesia to mitigate pain.
Gabapentin has been shown to reduce analgesic requirements and pain in women undergoing mastectomy. , Nonsteroidal anti-inflammatory drugs (NSAIDs) and cyclooxygenase-2 inhibitor medications are effective preoperatively or intraoperatively in reducing pain without increasing bleeding complications. Bupivacaine infiltrated into the area of planned surgical incision for mastectomy is also shown to decrease pain and opiate demand postoperatively. In addition, adenosine, systemic magnesium, venlafaxine, and clonidine are also effective analgesics when administered preoperatively.
Standard Anesthetic Protocol
Recommendation
General anesthesia with total intravenous anesthesia is recommended for breast reconstruction procedures.
There are 3 common modalities for maintenance of anesthesia during breast surgery: general anesthesia with total intravenous anesthesia, general anesthesia with a volatile anesthetic, and regional anesthesia. Regional anesthesia, with paravertebral or transversus abdominis plane (TAP) blocks, is shown to decrease postoperative narcotic use, but does not decrease pain, nausea, sedation, time to ambulation, or length of hospital stay. General anesthesia with total intravenous anesthesia decreases postoperative nausea and vomiting compared with a volatile anesthetic in breast surgery. ,
Preventing Intraoperative Hypothermia
Recommendation
Preoperative and intraoperative measures, such as forced air, to prevent hypothermia should be instituted. Temperature monitoring is required to ensure the patient’s body temperature is maintained higher than 36°C.
The Surgical Care Improvement Project found an association with hypothermia and impaired wound healing, prolonged hospitalization, and a 3-fold higher wound infection risk. Maintaining patient temperature higher than 36°C reduces multiple complications, including cardiac conditions, altered drug metabolism, as well as decreased wound infections. Preoperative patient-warming strategies affect intraoperative warming strategies, so warming an operating room will not be sufficient to prevent hypothermia. In a systematic review of multiple randomized controlled trials, forced-air warming is safe and effective in preventing hypothermia. Warmed intravenous fluid reduces hypothermia for short procedures, but in longer surgeries, it is insufficient.
Perioperative Intravenous Fluid Management
Recommendation
Overresuscitation or underresuscitation of fluids should be avoided, and water and electrolyte balance should be maintained. Goal-directed therapy is a useful method to achieve these goals. Balanced crystalloid solutions rather than saline is recommended. Vasopressors are recommended to support fluid management and do not negatively affect free-flap breast reconstruction.
Overresuscitation can affect cardiopulmonary events and wound infection and can increase wound-healing problems and length of hospital stay. , Both overresuscitation and underresuscitation have been shown to increase the risk of anastomosis thrombosis in free-flap breast reconstruction. , Historically, vasopressors used to maintain blood pressure have been avoided in flap patients, but studies have shown that they are safe to use in normovolemic patients. Balanced crystalloid solutions are shown to be superior to 0.9% saline for maintaining electrolyte balance.
Postoperative Analgesia
Recommendation
Multimodal postoperative pain management regimens that are opioid sparing should be used with the goal of facilitating early mobilization.
Consideration to reducing opioid use after surgery can help alleviate some of the effects of postoperative nausea and vomiting, as well as constipation. According to Cochrane data from randomized controlled trials, the combination of acetaminophen and NSAIDs is more effective than either alone. Multiple randomized controlled trials further demonstrate that NSAIDs reduce the need for narcotics with minimal surgical site bleeding risk. A metaanalysis of randomized controlled trials showed that ketorolac does not increase perioperative bleeding. Gabapentin administered preoperatively or postoperatively is effective for pain control and also demonstrates reduced narcotic requirements. ,
The use of regional or local blocks can help minimize pain, narcotic use, and sedation. Paravertebral blocks with continuous bupivacaine infusion catheters have been shown to reduce opioid requirements, , and TAP blocks have been effective in decreasing abdominal donor site pain in flap patients.
Early Feeding
Recommendation
Patients should be encouraged to take fluids and food orally as soon as possible, preferably within 24 hours after surgery.
Early refeeding within 24 hours after surgery is safe and associated with improved healing, reduced infection, and reduced hospital stay. The decision of when to resume a diet after surgery should be weighed against the risk of a possible urgent return to the operating room, for example, in patients who develop a microvascular thrombosis in their free-flap reconstruction. , Rapid-sequence intubation can help mitigate the risk of aspiration in the event of an urgent return to the operating room.
Postoperative Flap Monitoring
Recommendation
Flap monitoring within the first 72 hours should occur frequently. Clinical evaluation is sufficient for monitoring, with implantable Doppler recommended in cases of buried flaps.
Microvascular thrombosis of the free flap occurs in 2% to 5% of cases and typically within the first 72 hours. , , In most cases (60%–74%), thrombosis occurred in the venous system. , Studies have shown that the outcomes are improved in earlier salvage interventions in a compromised free flap. , Monitoring of flaps includes clinical observation for color, temperature, and capillary refill, as well as the use of monitoring devices. The hand-held Doppler is a noninvasive adjunct to clinical observation and is shown to be highly effective in monitoring free flaps. The typical protocol is 1-hour monitoring in the first 24 hours, every 2 hours for the next 24 hours, and then every 3 to 4 hours for the next 24 hours.
Implantable Doppler devices have excellent sensitivity in detecting flap compromise, but may detach and result in a higher false-positive rate than clinical observation. Clinical observation with or without implantable Doppler monitors has equivocal rates of flap salvage. , In the case of buried flaps, implantable Doppler is the only objective measure. Alternative flap monitoring devices include a venous coupler with an embedded implantable Doppler device, laser Doppler monitoring, infrared spectroscopy, tissue oximetry, and microdialysis.
Postoperative Wound Management
Recommendation
For incisional closure, conventional sutures are typically recommended. Complex wounds following skin necrosis are treatable with debridement and negative pressure wound therapy.
Typically, breast and abdominal incisions following breast reconstruction are closed with layered intradermal absorbable sutures. Skin adhesive octyl-2-cyanoacrylate is widely used in breast surgery and shows patient preference but no objective difference in cosmesis or complications. The length of time for a dressing to stay in place is variable. A clinical trial comparing dressing removal at day 1 versus dressing removal at day 6 is ongoing. Preliminary results may support standard recommendations of dressing removal after breast reconstruction in 24 to 48 hours.
Regarding complex wounds associated with mastectomy flap, DIEP flap and abdominal skin necrosis are known possible complications of breast reconstruction. , Surgical debridement and negative-pressure wound therapy is an effective adjunct in wound management, with studies showing complete healing in 97% of breast wounds.
Early Mobilization
Recommendation
Patients should be mobilized within the first 24 hours after surgery.
Prolonged inactivity combined with a catabolic state (ie, postoperative stress) exacerbates muscle atrophy. Early mobilization of patients improves muscle strength and reduces risk of pulmonary embolism, pneumonia, and decubitus ulcers. In addition, early mobilization decreases length of hospital stay and improves overall psychological well-being.
Postdischarge Home Support and Physiotherapy
Recommendation
Early physiotherapy, supervised exercise programs, and other supportive care initiatives should be instituted after discharge.
For patients undergoing mastectomy and axillary dissection, early physical rehabilitation has been shown to improve physical and emotional recovery. , Physical rehabilitation programs in the postoperative period improve mobility, decrease pain, and enhance quality of life for patients with breast cancer. Visiting nurses also provide an important role in delivering physical care and education, as well as psychosocial support following TRAM flap reconstruction.
The Johns Hopkins Enhanced Recovery After Surgery Protocol for Microsurgical Breast Reconstruction
The Johns Hopkins breast reconstruction team developed a protocol for microsurgical breast reconstruction that details the care elements based on the ERAS Society consensus report for microsurgical breast reconstruction ( Table 2 ). During the development of the protocol, multidisciplinary “buy-in” was first addressed through discussion with all members involved in the care of breast reconstruction patients at this institution, and all members came to a consensus based on evidence-based review of the literature. To highlight several specifications or modifications of the ERAS consensus report to the Johns Hopkins ERAS protocol, the preoperative analgesic regimen includes a combination of celecoxib, gabapentin, and oral acetaminophen. For antiemetic therapy, patients have a scopolamine patch applied in the preoperative holding area and may receive any combination of dexamethasone, ondansetron, or dimenhydrinate. Routine administration of 5000 units of subcutaneous heparin is given to patients in the preoperative holding area. Intraoperatively, TAP blocks are performed by the anesthesia team while the microanastomosis is being performed. Postoperatively, the diet is advanced in the morning after surgery to balance early feeding protocol and possible urgent return to the operating room in the event of flap failure.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


