Increases in opioid prescribing over the last several decades is correlated with an alarming increase in opioid-related morbidity and mortality owing to both prescription opioid misuse and abuse as well as heroin abuse. Prescribing after surgery is commonly in excess, and leftover pills are an important driver of opioid use disorders owing to diversion and misuse. Creating evidence-based prescribing guidelines based on patient-centered outcomes and encouraging safe opioid storage and disposal is critical to curbing opioid-related morbidity and mortality going forward and to ensure safe and appropriate postoperative pain management.
Key points
- •
Opioid-related morbidity and mortality have dramatically increased in the United States over the last several decades.
- •
Opioid prescribing after surgery has often been in excess, in part owing to the absence of clear prescribing guidelines based on patient-reported pain and opioid-related outcomes.
- •
Disposal of excess pills after surgery remains low, and unused opioid pills are an important contributor to the opioid epidemic owing to diversion and misuse.
Introduction
By numerous measures, opioid-related harm in the United States has been increasing over the past 2 decades. Rates of opioid misuse and overdose have reached new highs in recent years, fueled by an abundance of prescription opioids and new spikes in heroin and synthetic opioid use. Current estimates of the economic burden of the opioid crisis—including increased health care costs, productivity loss, and support from services such as law enforcement—top $100 billion per year. ,
The human and financial tolls of this crisis have stimulated a variety of responses from clinicians, researchers, community workers, and policymakers, many of which focus on the role of clinical prescribing. At the center of such initiatives are questions weighting appropriate pain management against patient and public safety, and of the responsibilities of the prescriber. The purpose of this article is to review the current state of the epidemic in the context of surgical prescribing and explore methods within the purview of the plastic surgeon to mitigate opioid-related harm.
An overview of the opioid epidemic
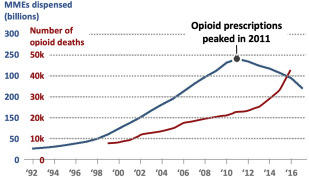
In 2017, about 68% of all fatal drug overdoses involved an opioid. This percentage represents 47,600 total opioid-related overdose deaths a year, or an average of 130 deaths per day. Opioid fatalities increased 12% between 2016 and 2017, reaching a number 6 times higher than in 1999, when opioid prescribing began to expand in response to concerted efforts to improve the treatment of pain , ( Fig. 1 A). Although the prevalence of prescription opioid misuse has significantly decreased since 2015, from 12.5 million to 11.1 million people, the number of people initiating misuse each year remains around 2 million (see Fig. 1 B). ,
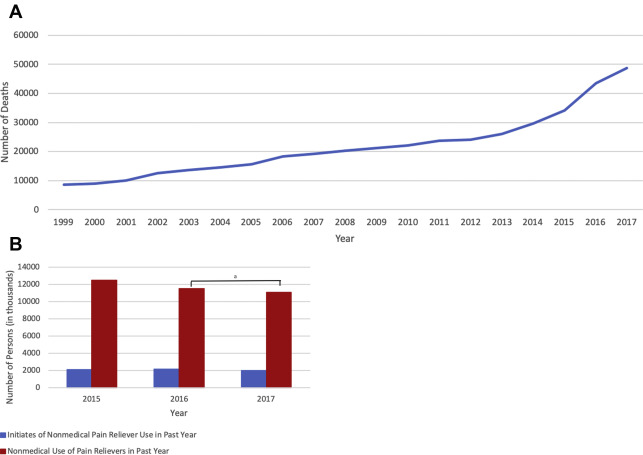
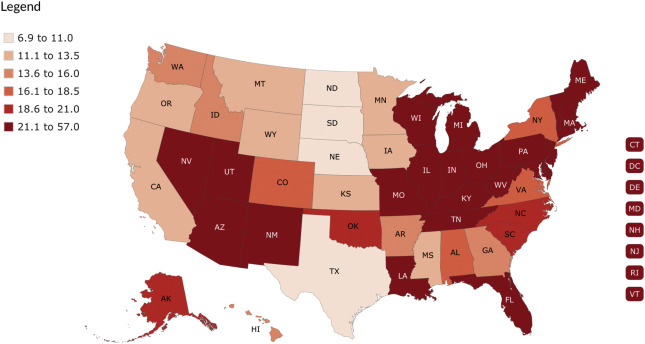
Rates of nonfatal opioid overdose are somewhat inconsistent with those of opioid mortality, having decreased by 15% between 2017 and 2018 for states represented by The Centers for Disease Control and Prevention’s Enhanced State Opioid Overdose Surveillance program. Still, several individual states still reported increases in nonfatal overdoses during the same time period, and rates again began to increase throughout the beginning of 2018 for all states. Rates of opioid overdose throughout 2016 and 2017 varied almost 3-fold among US regions with the highest rates observed in the Northeast, followed by the West, Southeast, Midwest, and Southwest ( Fig. 2 ). In the same time period, the mortality rates in urban settings have remained stable, whereas those in rural areas have decreased, lessening the gap between the two. Factors confounding urbanicity, such as economic distress, opioid supply, and race or ethnicity may be better predictors of geographic variation in some cases. This variability suggests that smaller, regional analyses may be necessary to capture the sociodemographic nuances of this epidemic and offer opportunity to identify targets and processes for reduced morbidity.
The role of perioperative opioid prescribing
Of the many opioid overdose deaths in 2017, 35% are attributed to prescription opioids specifically. Moreover, use or misuse of prescription opioids remains the most common exposure to later heroin use. , These figures highlight the significant contribution of clinical prescribing to the opioid epidemic, and continuous review and revision of prescribing practices is critical to minimize risk to patients and the community.
Patterns of Opioid Prescribing
Historically, the rate of fatal opioid overdoses closely paralleled prescribing rates. Notably, in 2011, prescribing rates began to decrease, owing to the combined effects of legislative regulation, clinical guidelines, financial controls, and increased national attention, which have encouraged or mandated changes in clinical practice, among other things. However, overdoses continued to increase at a greater rate beyond 2011, fueled predominately by heroin and synthetic opioids, such as fentanyl and tramadol ( Fig. 3 ). The national rate of prescribing has continued to decrease through 2017. From 2016 to 2017, the total opioid dosage filled saw a 12% decrease, the largest single-year decrease in 25 years. However, more nuanced analyses have shown that prescribing in a handful of practices—including surgical, dental, and emergency care—has continued to increase from 2010 to 2016, despite the national downturn. Surgery in particular had an increase of nearly 70% in average total morphine milligram equivalents prescribed in this time period, and in 2016 surgery patients filled the most opioid prescriptions out of these 3 specialties.
In addition to quantity, the types of opioid prescribed are also important to consider, given that increasing potency is correlated with a higher frequency of adverse events. Hydrocodone and oxycodone, which are very commonly used for postoperative analgesia, account for the majority (77%) of serious adverse events, including death. Nevertheless, between 2013 and 2015, oxycodone prescribing dramatically increased, , translating into a greater number of patients exposed to this potent formulation. In the same period, 1 institution found that the frequency of tramadol prescriptions increased along with oxycodone after various procedures, a shift that coincided with the rescheduling of hydrocodone in 2014 prohibiting phoned prescriptions to pharmacies. Notably, patients undergoing surgery are particularly more likely to receive oxycodone and hydrocodone as compared with dental or emergency care patients.
Overprescription of Opioid Analgesics
Increasing rates of opioid prescribing within surgery are concerning, but more notable is the growing body of literature to suggest that opioids have been markedly overprescribed for postoperative pain management for decades. For example, Hill and colleagues reported that more than 70% of opioids prescribed after common surgical procedures remain unused. In addition, in a systematic review of 6 studies on opioid prescribing and use, as many as 71% of opioid pills dispensed to surgical patients went unused, and as many as 92% of patients had pills leftover from their postoperative prescription.
Other studies report median prescription sizes that are 2 (in outpatient plastic surgery procedures) to 5 (in abdominal procedures) times greater than patients actually use. , Prescribing is not only excessive, but also highly variable, even after the same procedure type, perhaps indicating that prescribing is not consistently anchored by specific evidence. These findings suggest that both standardization and reduced prescribing are appropriate steps for surgical providers to reduce the amount of leftover opioids.
Although reduced postoperative opioid prescribing may raise concerns surrounding inadequate pain control or lower patient satisfaction, there is already growing evidence suggesting that these measures do not suffer when patients take fewer pills. , , A recent study of outpatient plastic surgery procedures found that prescription size was not significantly correlated with patient satisfaction. Further, the top reason that patients reported not consuming the opioids prescribed to them, other than experiencing adverse events, was the ability to achieve adequate pain control without opioids. Although the amount of opioid prescribed and consumed have both independently been correlated with pain scores, , Howard and colleagues noted that one of the strongest predictors of the amount of opioid consumed among surgical patients is the prescription size provided after surgery. Recognizing that a larger prescription may influence patient behavior in taking opioids, and that appropriate pain control and patient satisfaction are achievable with limited use of opioids, it is critical that surgeons take a judicious approach to postoperative opioid prescribing.
Storage and Disposal of Leftover Opioids
Unused opioids leftover from prescriptions are available for misuse or diversion, especially if they are not stored or disposed of properly. Despite these risks, rates of medication disposal are consistently low, and those that do dispose do not do so in alignment with guidelines from the US Food and Drug Administration. Moreover, about three-quarters of patients report storing their opioids in unlocked locations, such as a cabinet or on a kitchen counter. These poor practices may represent a gap in provider education surrounding safe storage and disposal practices. For example, in a poll of adults ages 50 to 80 years of age who had been prescribed an opioid in the last 2 years, just 37% recalled receiving disposal instructions from their surgeon or health care team, and in another study only 18% of patients reported receiving such education. Given the risk for diversion and misuse, it is important to not only match prescribing more closely to need, but also to educate patients on the proper storage and disposal of opioid medications.
Besides lack of appropriate counseling, barriers to disposal options outside the home (eg, law enforcement drop box, medication take back event) may also contribute to the failure of patients to dispose of leftover opioids. Brummett and colleagues reports that providing patients with an activated charcoal bag for in-home medication disposal significantly increased the probability for disposal of unused medication, as compared with patients who received usual care or disposal education alone. Provision of materials for in-home disposal along with opioid prescriptions is a promising method to further promote safe disposal of medications.
New Persistent Use and Misuse after Surgery
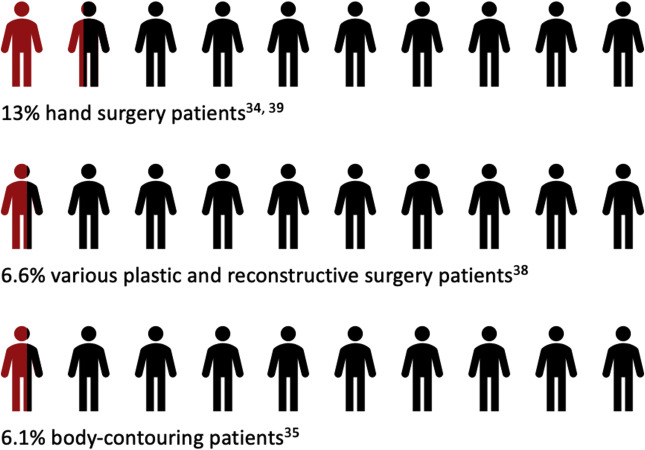
New persistent use (NPU) is a significant risk of perioperative opioid prescribing. Although NPU has been defined in a variety of ways, this is commonly considered to be continued opioid fills after 3 months after the index procedure in the absence of additional surgical procedures among opioid naïve patients. Estimates of the prevalence of NPU vary by procedure type and specialty. Various studies report the rate of NPU for opioid-naive patients to be anywhere from 4% to 15%, including in pediatric general surgery procedures. Studies on plastic surgery procedures in particular report rates at the higher end of that range, with 6.1% of patients undergoing body-contouring procedures, 6.6% of patients having various plastic and reconstructive procedures, and 13% of hand surgery patients , meeting criteria for NPU ( Fig. 4 ). Additional studies suggest that rates of NPU vary between operating room and nonoperating room procedures, as well as elective versus trauma surgeries. Given that complications after most surgical procedures are relatively low, NPU is a common and important complication after surgical care.
Importantly, there are a number of factors that increase the risk of NPU among opioid-naive patients, including alcohol and substance abuse diagnoses, mental health disorders (anxiety, depression), tobacco use, and pain disorders. For adolescents and young adults, long-term opioid use in a family member is associated with increased odds for persistent use after surgery. Also, new persistent users are more likely to be younger, female, lower income, and have more comorbidities. Attention to these patient-level factors is particularly warranted in light of the findings by Brummett and colleagues that NPU is associated more strongly with patient-level predictors rather than the severity of a procedure.
There are also factors associated with higher rates of NPU that are at the discretion of the provider. Body-contouring patients that were exposed to high-risk prescribing practices (which include prescriptions of >100 oral morphine equivalents per day, of long-acting opioids, from >1 prescriber, or that overlap with benzodiazepine or other opioid prescriptions) were more likely to be new persistent users as compared with those patients who were not exposed to such practices. These findings are consistent with other studies that have demonstrated that each refill and additional week of opioid use are associated with a higher adjusted rate of misuse, that increasing total OMEs are associated with increased risk for NPU, and that long-acting opioids increase the risk for NPU compared with short-acting formulas. , Avoidance of these high-risk practices, and careful consideration of patient-level risk factors, should accompany perioperative opioid prescribing.
Transitions of Care After Surgery
In considering NPU, the question arises of who continues to provide opioid prescriptions long after the postoperative period. A retrospective study of national insurance claims found that although surgeons were responsible for the majority (69%) of prescriptions to opioid naive patients in the 3 months after surgery, they only accounted for 11% of prescriptions 9 to 12 months after surgery. In contrast, primary care providers prescribed 13% in the first 3 months then 53% in postoperative months 9 through 12, emergency medicine accounted for 2% then 5%, physical medicine and rehabilitation 1% then 6%, and all other specialties 15% then 25%. These findings suggest that although NPU starts with a surgical prescription, primary care providers and other specialists are majorly responsible for the continuation of the provision of opioids. Surgeons should therefore take steps to better facilitate transitions of care for patients discharged with an opioid prescription, so as to monitor for misuse and NPU.
For opioid-exposed patients and those with chronic opioid use before surgery, facilitating transitions of care with other prescribers is an important step in minimizing exposures to high-risk prescribing practices. As reported by Lagisetty and colleagues, 10% of such patients do not have a consistent prescriber before surgery and are thereby at increased risk for exposure to high-risk prescribing practices (eg, receiving prescriptions from multiple providers). Of the 90% that do have a usual opioid prescriber, return to that provider within 30 days postoperatively is associated with a decreased risk for multiple prescriptions.
Efforts toward safer prescribing and use of opioids
The Legislative Response to the Opioid Epidemic
Policymakers at both state and national levels continue to pass regulatory measures to reduce opioid-related harm. Much of this effort has been reactive, focused on improving outcomes for those already struggling with opioid use disorders or experiencing overdose. For example, the Federal Drug Administration is working to increase access to naloxone, an opioid antagonist that can reverse the effects of opioid overdose, in the hopes of reducing fatalities. Access to Medication Assisted Treatment programs has improved with the passage of the Patient Protection and Affordable Care Act—which mandated that marketplace plans cover substance abuse treatment—by the expansion of coverage of these services for eligible Medicaid recipients, and increasingly by federal grants awarded to individual states to expand Medication Assisted Treatment services. Experts believe these policies are responsible, at least in part, for the declining rate of overdose deaths by prescription opioids in recent years.
Additional policy measures protect overdose victims and those who seek help on their behalf from legal repercussions, promote data collection on drug overdoses and fatalities, and discourage illegitimate prescribing of controlled medications. , More germane to surgical practice, there are several legal measures, which often vary by state, that directly impact providers’ prescribing practice.
Preoperative counseling
Some recent mandates, such as Public Acts 246 and 248 of 2017 in Michigan, and institutional policies require that prescribers provide patient counseling before issuing a prescription for an opioid. Such education may communicate the risks of opioid use, expectations for pain, and alternative modalities for pain control. , A prospective study of carpal tunnel release patients (n = 40) suggests that this practice may have merit in decreasing postoperative opioid consumption. Patients randomized to a group receiving formal preoperative counseling reported taking significantly fewer pills than patients in the control group who did not receive the counseling, despite receiving the same number of opioid pills. There was no difference in reported pain scores. Based on these results, the authors recommended that surgeons incorporate preoperative counseling into routine practice, an assertion supported by a number of other experts in the field. , ,
Prescription drug monitoring programs
As of 2017, prescription drug monitoring programs (PDMPs) have been authorized for creation and use in all 50 states and the District of Columbia. PDMPs are valuable tools in identifying situations of potential opioid abuse, because they allow prescribers and pharmacists to view patients’ prescription histories. Owing to this central function, they have been leveraged in a handful of states to decrease inappropriate opioid prescribing. For example, New York and Tennessee experienced significant decreases in doctor shopping after a 2012 mandate required providers use the states’ PDMPs. Despite this and other evidence that PDMPs have the power to reduce high-risk prescribing and consumption patterns, their impact is limited by inconsistencies in use, the lack of connection between state systems, and prompt data updates.
Prescribing limits
A number of states and individual organizations (eg, private health insurers, retail pharmacy, pharmacy benefit managers, health systems) have recently enacted opioid prescribing limits, generally capping prescriptions at a 3- to 7-day supply. , The goal is to curb excessive prescribing, which would limit opioid exposure for first-time users and minimize the amount of leftover prescriptions. Skepticism remains, however, over the potential impact of this approach. Some critics have pointed out that a one-size-fits-all restriction will likely not be effective for a heterogeneous patient population, in which individuals have unique pain experiences and histories with opioid use. The mandated limit may be too low for some patients, impeding adequate pain control, , while being too high for others, rendering the laws ineffectual in limiting prescribing to need.
Additionally, broadly applicable limits must allow for a large number of exceptions to accommodate a variety of unique circumstances without introducing so much flexibility as to undermine the intention of the regulations, a balance that could be difficult to achieve. Already there may be loopholes in these policies that allow physicians to circumvent the new limits. For example, a physician may prescribe higher doses within the daily limit, but direct patients to take fewer pills per dose over a longer duration, or they may forward-date an additional prescription to bypass restrictions on opioid refills. Experts predict that detecting or mitigating this type of activity would be challenging. Ultimately, these potential difficulties lead some to believe that sweeping prescribing limits will be ineffective in achieving their intended goal.
Prescribing Guidelines and Best Practices
Regardless of legislation, it is ultimately incumbent upon the surgeon to use strategies that mitigate potential risks to patients and the community. To do this, providers may need to adopt additional precautionary practices outside of those mandated by law or by institutional policy. Besides the measures already discussed—including preoperative counseling, consistent use of PDMPs, and patient education on disposal methods—evidence and experts agree that prescribing guidelines and the use of nonopioid analgesics for postoperative pain may also be effective in curbing unnecessary prescribing , ( Fig. 5 ).