Introduction
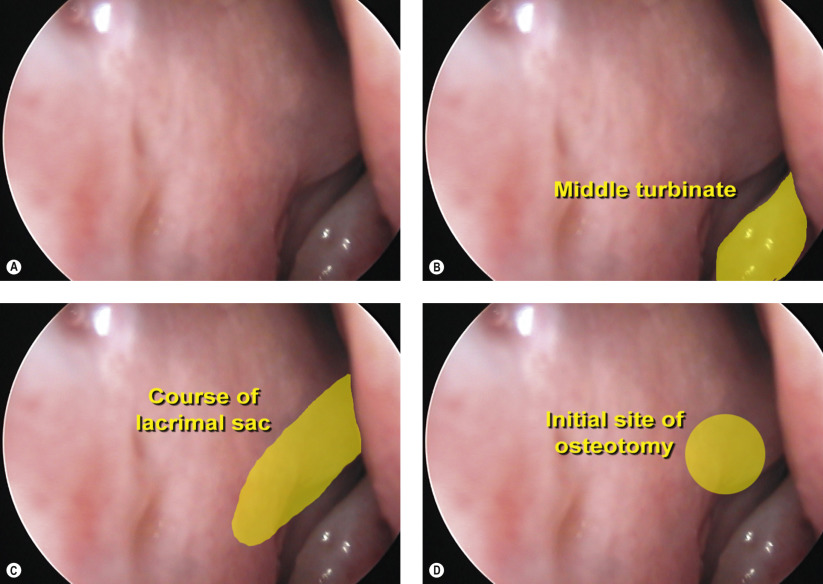
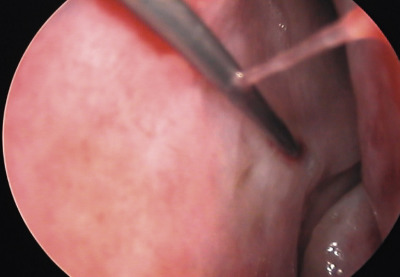
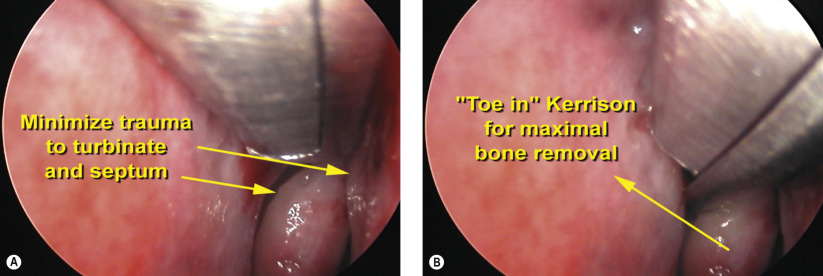
In this chapter, endoscopic dacryocystorhinostomy (DCR) with the use of an osteotome is presented. For indications and preoperative evaluation, refer to Chapter 53 . The osteotome is a useful adjunct during endoscopic DCR to rapidly remove the difficult-to-reach bone at the superior portion of the lacrimal sac fossa. Once the lacrimal sac has been exposed using the Kerrison ronguer, the 6 mm osteotome is directed vertically to fracture the frontal process of the maxilla along the lacrimal sac fossa. Once the vertical osteotomy has been completed, the osteotome is rotated horizontally to fracture the remaining thin lacrimal bone. The entire maxillary–lacrimal complex encompassing the lacrimal sac fossa can often be removed as a single unit.
Surgical Technique
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


